Interaction Report: Acute Gastritis
Jan 1, approx. 11:45 PM - Jan 2, approx. 2:00 AM
Your epigastric pain has persisted for 2 hours with zero mitigation.
You describe the symptoms to an AI; the AI alerts you that you have exceeded the Home Safety Threshold.
Your consciousness is clear, so you decide to execute an immediate jump to the ER.
You dress, hunch over, and shuffle out the door (because the pain makes upright walking impossible).
Your avatar looks like a boiled shrimp, an atavistic ape, a zombie from Plants vs. Zombies.
You successfully hail taxi, speeding toward a Level-3 General Hospital.
You enter via the main gate, forcing a brisk walk into the emergency building.
You see the Registration Window.
So, you walk over to register.
......
OK, this is just the beginning.
This is the first time in my limited lifespan that I have voluntarily initialized a hospital visit; I have never entered this map before.
It is also this unbearable pain that has forcibly dragged me into the most sophisticated, yet most absurd system in the real world:
The Emergency Department of a Level-3 General Hospital.
If Kafka were this system’s initial Product Manager, then what you are about to see is likely the “Final Stable Build” after a century of iterations.
Here, suffering is not flagged as high priority; data integrity is.
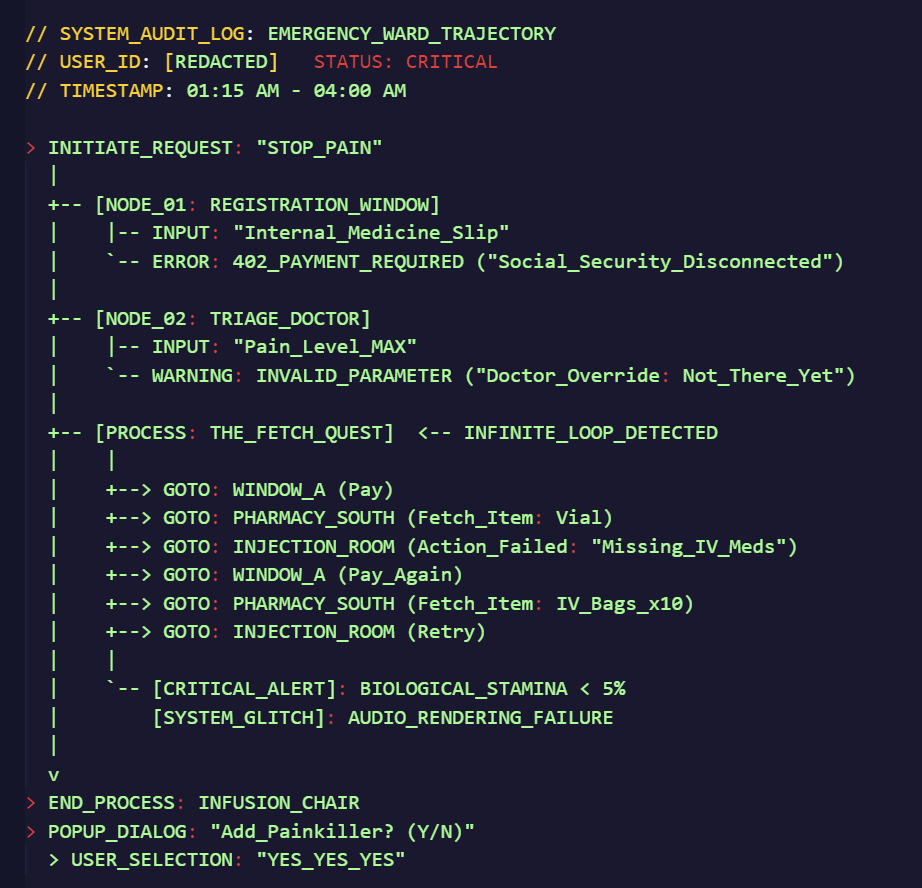
My user requirement is simple: Terminate Pain.
But in the system’s logic, this is an Illegal Request.
The midnight ER hall is quiet and bright. [UI Layer: Emergency Registration Window] appears in the field of view first. Two windows, one displaying “Running.”
I drag my feet toward the active window. The glass is clear, looking almost organic.
The voice from inside sounds like a pre-recorded audio file: “Go to Triage first.”
I leave the window, dragging my feet again into the hall. [Verification Layer: Emergency Triage].
The nurse asks how/what/where it malfunctions.
I say: “Epigastric pain, center, can’t stand up straight.”
The nurse and the doctor on duty tell me to sit. They check my blood pressure (no result communicated). I’m handed an “Internal Medicine” triage ticket: “Go to emergency window to register.”
I stand up, arching my back—no need for cosmetic skins, I’m naturally an atavistic ape—and drag my feet back to [Payment Layer: Emergency Registration Window], sliding in the ticket.
Voice from the window: “Name, Age, Company, Address, Door Number.”
I pause to gasp for air after every phrase.
The counterpart assumes I refuse to input data and prompts: “Creating a file for you.”
Then, the System Error audio plays: “Your Health insurance payment has been interrupted. You can swipe the card, but you can’t be reimbursed. Do you know that?”
The severe pain is occupying 100% of my brain’s computing power. I can’t parse what specific outcome these words point to; they flow straight through my brain and into my stomach.
What I’m thinking: Pay, Diagnose, Stop Pain.
However, the system doesn’t care who I am; it only cares about my “Subscription Status.”
This is the first time I realize that as a biological user, my permission level is lower than the database.
Middle of the hall, right side. Internal Medicine Consulting Room.
I sit by the desk, arm resting on the table, head down, selling my effort to breathe.
The doctor sits behind the monitor, commencing standard Metadata Collection and verification:
“xxx, is that your name?”
“How old?”
“Married? Pregnant? Preparing for pregnancy?”
“Last period date?”
These questions float in the air, a pile of garbled code.
I give mechanical responses: Yes, right, no, no, no, I forgot.
I attempt to input core failure information amidst the garbled code: “Upper abdomen, middle section, hurts like death.”
The doctor immediately intercepts the packet, denying it three times: “No, no, no, not there yet.”
I shut my mouth.
He refuses to acknowledge my pain level.
In his diagnostic manual, I haven’t triggered the “System Crash” threshold yet.
I don’t possess the administrative rights to interpret my own pain.
The doctor asks me to lie on the examination bed. “Now I’ll check the abdomen. Tell me when I press somewhere that hurts.”
After a string of ‘No’s, he presses on my upper center abdomen. Cold sweat instantly pops on my forehead, and I yell: “Hurt!”
For the next hour, I enter the Death Stranding instance, only without the exoskeleton—just a malfunctioning meat-suit liable to shut down at any moment.
This is a path designed to punish the “weak.” The system assumes a “Single User” cannot initiate an ER session independently; it defaults to the requirement of a Healthy Companion (preferably a Family Unit).
I guess the logic is: If your case is critical, you can’t come alone; if you come alone, your case isn’t critical.
Every step here is testing my willpower. Fortunately, willpower is something usually useless that only works at critical moments.
Item Acquired: Internal Med doctor prints a string of lists. Diagnosis: Acute Gastritis. 1F Intramuscular Injection, 2F Blood Test, 3F Ultrasound. But first, go to Emergency Window to pay.
Recall: This is my third return to the Emergency Window. Payment initiated.
Instance A: I drag my steps past Triage, past Internal Med, to the Injection Room at the far end (Southeast corner) of the 1st floor. Nurse glances at the list: “Go get the meds from the pharmacy first.”
Instance B: I let out a long breath, my avatar morphing from Zombie to Walker. Turn around, exit, pass fire doors, pass elevator, walk to the South Pharmacy in a separate building. Retrieve a glass vial the size of a pinky finger.
Return to Instance A: Back to Injection Room. Injection administered.
Instance C: Walk to the elevator. Elevator out of service. I clutch the papers and climb the stairs. Squat on the floor to queue. Blood draw.
At this point, my spirit begins to dissipate.Auditory system glitches; I can’t hear human volume levels.
Phlebotomist presses a cotton swab on my finger, raising the volume: “Hold it yourself.”
Instance D: Continue climbing stairs. Queue. Smothered in coupling gel. Asymptomatic gallstones detected. I wipe off the gel and scramble off the bed. Doctor says: “No rush.”
I hunch over and say: “My stomach is killing me.”
Coming down from the 3rd floor, I can’t walk in a straight line. Every few steps, I have to find a corner to squat in. Mind blank. Eyes seem to see clearly, yet register nothing.
I take the Ultrasound result back to the Internal Med room in the middle of the hall.
I’m back at this coordinate, doubting if I ever left.
Intramuscular injection ineffective. Pain unmitigated.
Doctor suggests upgrading the treatment plan (IV Drip).
I feel like a computer failing to reboot, gasping: “Fine. Just stop the pain.”
So, I Blue Screen and reboot, looking like I’m hiding some unknown virus, struggling to enter the next Instance:
Return to [Verification Layer: Emergency Triage]: Redirect. Get Surgery Dept ticket.
Return to [UI Layer: Emergency Registration Window]: Re-register. Register for Surgery. Pay.
Go to Surgery Clinic: New round of interrogation. I drag my feet to the far left of the 1st floor hall. Another doctor, also behind a monitor, asking the same questions. “Name? Age? I saw your tests...”
I no longer remember what I answer, probably just a few grunts.Return to [Payment Layer: Emergency Registration Window]: I hand the IV slip from the Surgeon into the window. Fourth Payment. The person inside has changed (shift change, maybe).
The System Error audio plays again: “Your Health insurance payment has been interrupted. You can swipe the card, but you can’t be reimbursed. Do you know that?”
Go to Emergency Injection - South Pharmacy: Fetch Quest Triggered. Yes, I went to the Injection Room first again, and was reminded again: ‘Go get the meds from the pharmacy first.’
I hold the payment receipt and retrieve a huge pile of IV medications, so many I can’t hold them in two hands and have to carry them in my arms.Return to Emergency IV Room: Finally. I sit on the IV chair, hard as a rock, clutching a stack of crumpled receipts, residue chewed up and spat out by the system.
In the short time waiting for the needle to pierce the back of my hand, the most ironic pop-up appeared.
The nurse shouted from the prep room: “xxx, do you want to add painkillers?”
In that instant, I suddenly thought of the donkey at the mill. The donkey chases the carrot, grinding for a whole day until its four legs give out and it’s crawling on the ground. Only then does the owner, in a fit of mercy, toss the carrot right in front of its eyes.
I had been circling in this system just like that. One second before I passed out, it suddenly displayed its “Humanized Configuration.”
I also shout: “Add. Add. Add. I’m dying.”

Sitting in the IV chair, I slept through the process. The 4 AM timestamp and the ceaseless pain exhausted me.
I returned home. It took three days of recovery before I could stand straight and walk upright.
Sitting on the sofa looking at the bruise on the back of my hand, the scene of the emergency building returned to my mind.
Only then did I realize: the ER at dawn was empty. There was no shortage of medical resources. It was purely the arrogance of interaction design.
The hospital’s spatial map and workflow are designed based on the stamina and logic of a “Healthy Person.”
The Administrator assumes the user possesses full mobility, clear cognition, and sufficient patience.
But in an ER scenario, the User (Patient) is defined precisely by the loss of these capabilities.
Too painful to walk -> Must walk to every node -> Go to every node to stop pain -> Must walk to every node before stopping pain.
As I said earlier, the System default is: If you can’t complete these dozen round-trips independently and give up halfway, your failure severity isn’t high enough; if you can finish the run, you aren’t that sick.
This is a perfect logical closed loop, only with the variable “Suffering” removed.
In that massive white maze smelling of disinfectant, the concept of ‘Human’ is skillfully dissolved.
Triage, Registration, Payment, Blood Draw, Clinics, IV Room, Pharmacy, Ultrasound... everyone does their job, real-time sharing my data.
My name and ID are the only index; the receipt is the only token.
As for the meat-suit bent over in pain, just a biological carrier used to transport the receipt from Window A to Window B.
The system runs flawlessly. Sometimes it even includes black comedy. Like, “Do you want to add painkillers?” Can you say that’s not humorous?
The only thing that crashes is the person serving as “consumables.”
When a human becomes a biological modules, dignity is lost.
I love reading novels. I always thought I could write some stories, but actually, I can’t write at all.
Dystopia, Sci-Fi, Absurdism, Existentialism, Cybernetics, Systems Theory, Simulation Theory, Information Theory... studying these things seems useless because I was fantasizing about something based on ‘human’ logic. It’s simply ethereal.
True horror is banal.
Reality is the craziest author.
It only needs to wait until you are bent over in pain to say to you:
“Go to Triage.”
“Go to Window to Pay.”
“Go to Pharmacy to get meds.”
......
Go.
Go.
Go.
— Wider. Freer. Suggger
Read the original article
