
2.5k words, 12 minutes reading time
Edit on 08/06/2024: At least one person has pointed out that, at one point, giving hypertensives at night were also thought to matter, a now disproven idea. Someone also mentioned how many times the clinical trial information was altered during the study. I added in a section at the end to discuss this.

There’s a really interesting phenomenon in the immunotherapy field that has been going on for what seems to be several years now, but was raised to me — a non-oncologist — via a viral Twitter thread of some work at ASCO25:
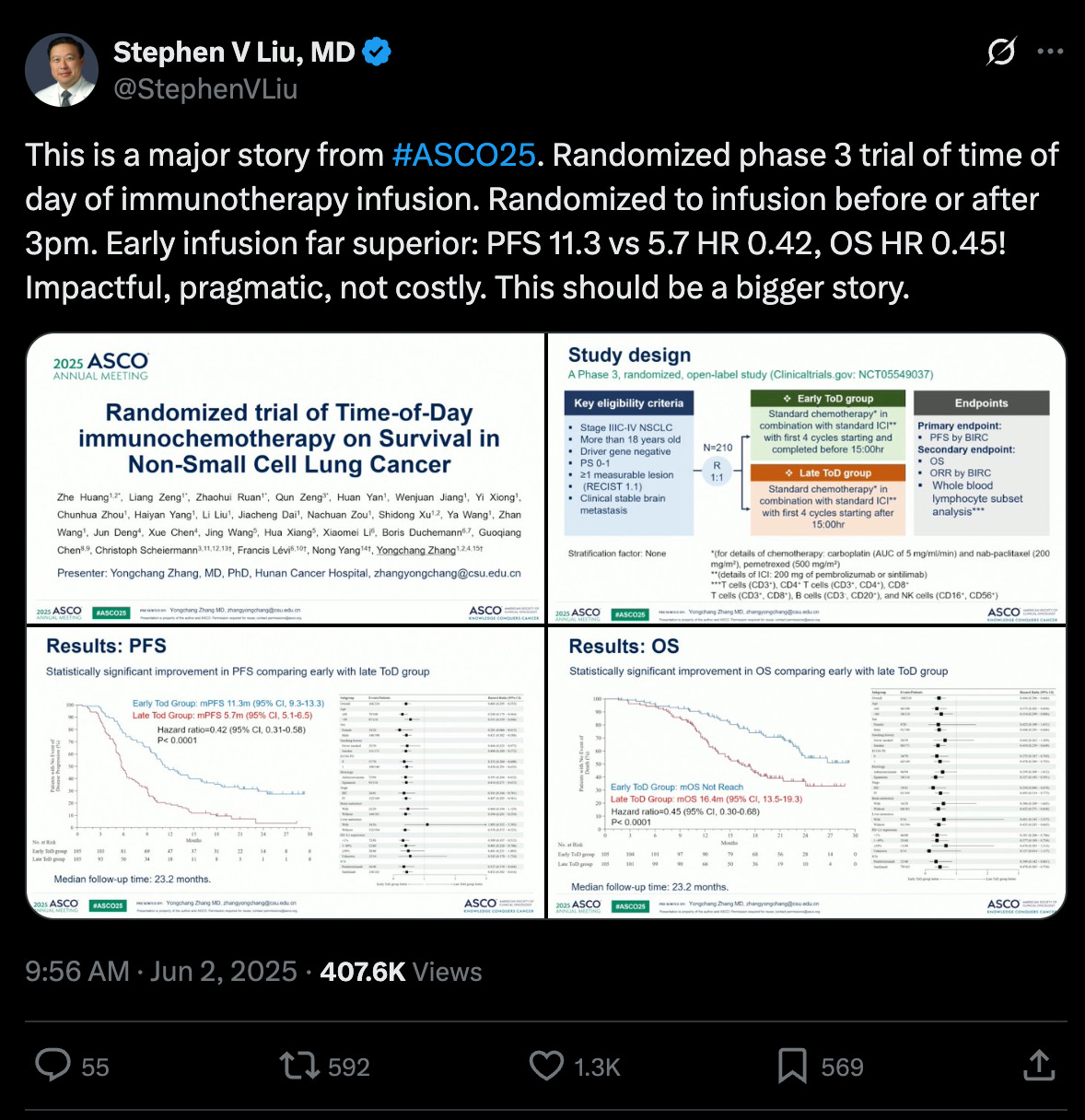
Translating the jargon: amongst the patients who received their immunotherapy infusion before 3pm (as opposed to after 3pm), their cancer stayed under control for longer (11.3 months vs. 5.7 months) and on median lived longer (at least 23.2 months versus 16.4 months). A near 2x~ improvement in the most important metrics doing something that is entirely risk-free and cost-free.
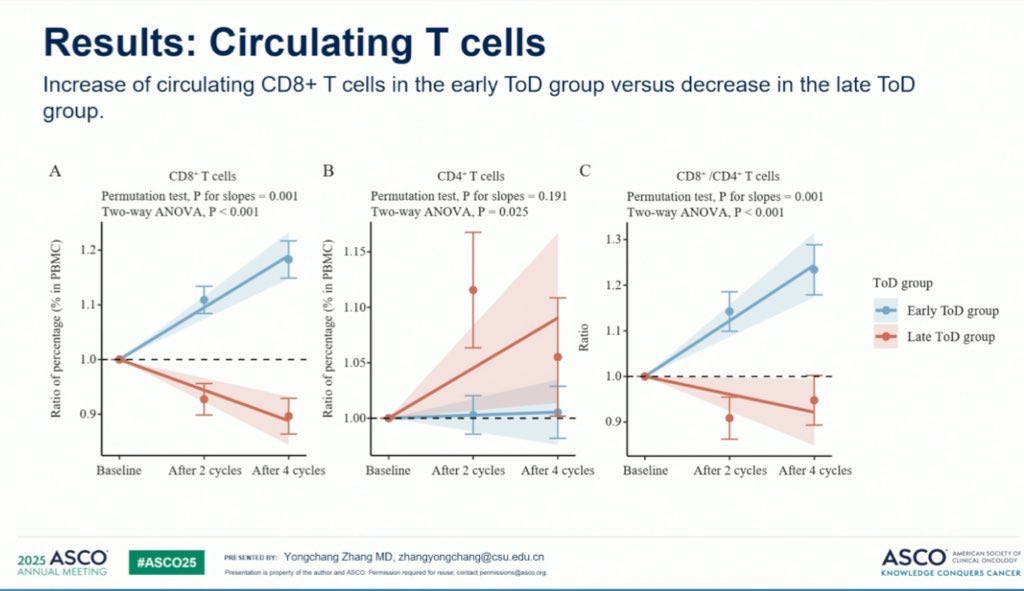
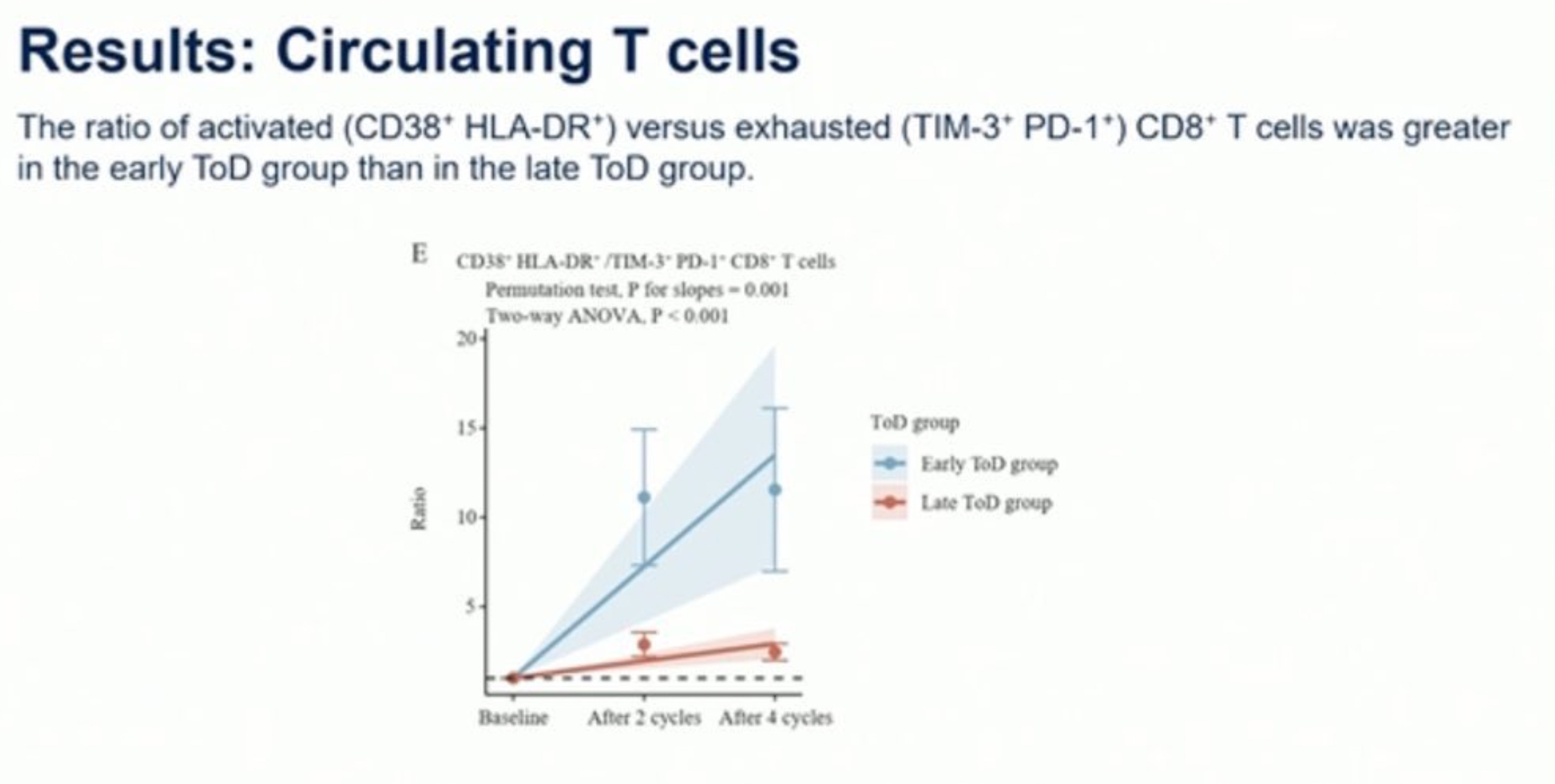
These two images shown in the comments of the post also demonstrate genuine changes in levels of circulating T-cells between the two groups:
Important context: the current standard of care for immunotherapy is not designed with timing in mind. You come in to get the injection when convenient for you or when there are free spots, there is no official recommendation to get it in the morning. But this study implies that we should potentially update our guidelines.
Weird, right? And if you have my relatively naive instincts, obviously wrong. Something must have been off in the study. After all, wasn’t there that one paper about how time-a-lab-test-is-taken is more predictive of patient survival than the test results themselves? The punchline? Sicker patients have strangely-timed emergency lab orders at 2AM, healthy patients have routine morning blood draws. Timing is hard to rely on!
But this paper was not a retrospective study of electronic health records, it was a randomized clinical trial, which is the gold standard. This means that we’ll be forced to immediately throw away our list of other obvious complaints against this paper. Yes, healthier patients may come in the morning more often, but randomization fixes that. Yes, patients with better support systems may come in the morning more often, but randomization fixes that. Yes, maybe morning nurses are fresher and more alert, but, again, randomization fixes that.
Okay. Well. Maybe there is something here. Caveats on this of course being a conference presentation without a corresponding, longer peer-reviewed paper, so we lack a lot of exact details on what exactly went on. Maybe the randomization used here is off for some reason, we’ll see once an official paper comes out.
But perhaps we should look beyond just this research. As it turns out, there is an astonishing amount of pre-existing literature on the immense benefits in giving patients immunotherapy earlier in the day, also known as ‘immunochronotherapy’. The exact time varies, but anytime before the evening seems to be good. Here’s one study that found, again, a massive improvement when giving immunotherapy before 11:30AM for advanced non-small cell lung cancer. And again for esophageal cancer, before 1pm. And again for melanoma, before 4:30.
All of this culminated in a really incredible review paper that is really worth reading. It walked through 18 retrospective studies covering 3,250 patients, each of which studied the impact of immunotherapy injection time on patient outcome. And, once you compile them all together, there is a very dependable story being told across multiple types of cancer.
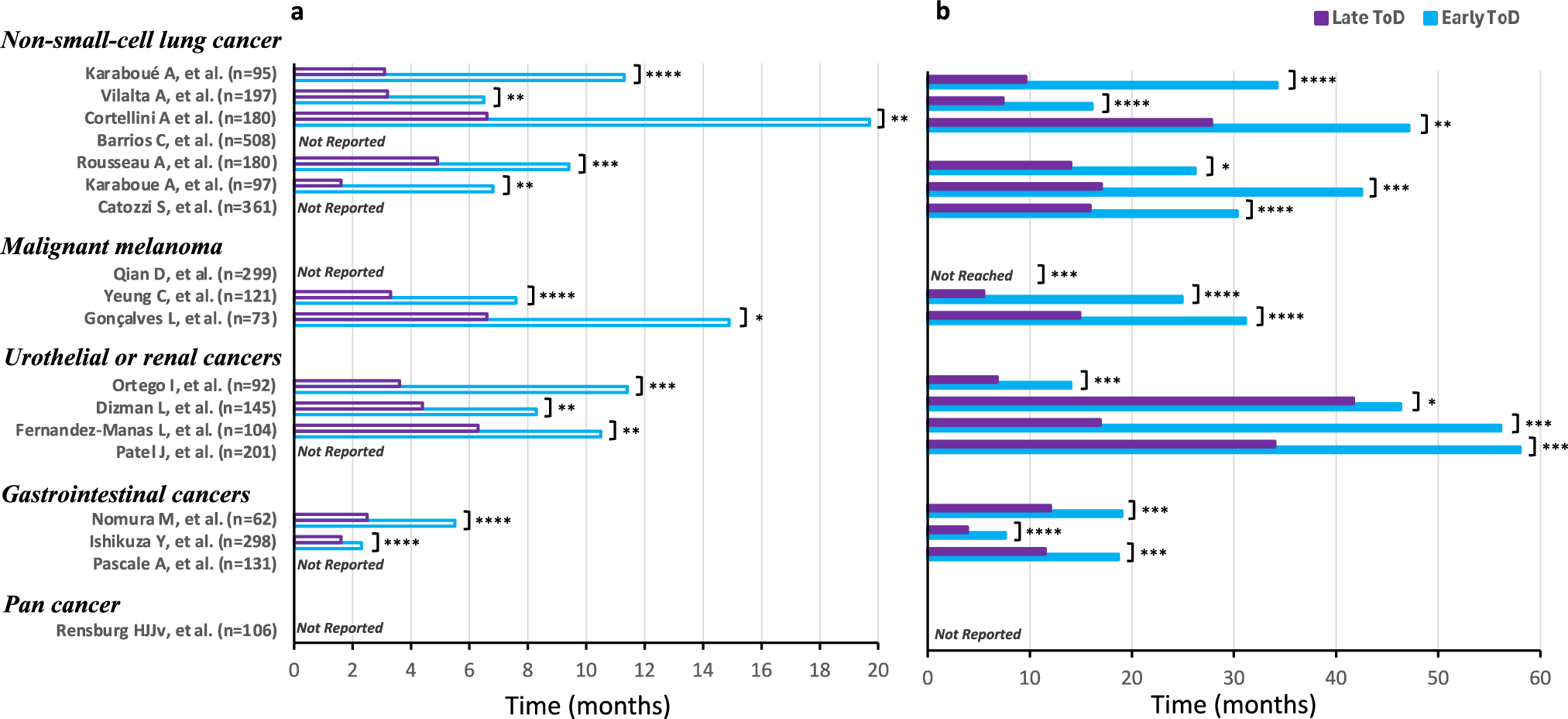
TLDR: early-in-the-day immunotherapy administration consistently leads to massive improvements in survival time, matching up quite well with the 2x results from the original Twitter post.
Keep in mind, these results have not only been shown for short-lived small molecules, but also long-lived proteins with half-lives on order of weeks that shouldn’t be affected by 24-hour cycles: pembrolizumab (Keytruda), nivolumab (Opdivo), and ipilimumab (Yervoy). Now, skepticism here would be justified given that these are all retrospective studies, and it’d be very easy for these to be confounded. But this evidence combined with the extremely similar results from the randomized clinical trial done I showed at the start of this essay should lead us towards at least suspecting that this is an honest-to-god free lunch.
What’s going on? Where is this coming from?
First, it’s worth reminding ourselves that the human body — and perhaps most complex life on Earth — exists on a schedule: the circadian rhythm. There exist 15-or-so ‘clock’ genes, like BMAL1, CLOCK, PER, and CRY, that oscillate with a rhythm. Not in structure or conformation, but in expression; the amount of them present in cells rises and falls over the course of the day. BMAL1 and CLOCK form a complex that drives the expression of PER and CRY. Once PER and CRY accumulate to a certain threshold, they feed back to inhibit BMAL1 and CLOCK, suppressing their own production. Over time, PER and CRY degrade, releasing the inhibition, and the cycle begins again.
One full loop takes just about 24~ hours, though there is some degree of individual variation.
So our cells have evolved to take advantage of these genes as an internal timestamp, a marker of where we are in the circadian rhythm. Some things occur early in the cycle, some things occur later, purely as a matter of convenience.
What’s the point of the cycle? One way to understand them is through an evolutionary lens, a way for the body to prepare for dependable environment cues.
For example, at the start of our circadian rhythm, we wake up. We crawl out of our safe cocoon — a private bed in modernity, or a predator-sheltered hole in ancient history — and start to engage in very risky behavior, immunologically speaking. Eating leftover food that may be contaminated, being scrapped by bacteria-covered rocks, holding dead animals to roast for dinner, and so on. But, as night comes, we retreat back to our private beds or holes, feasting on freshly cooked food, few interactions with unknown creatures, and little chance for injury as we wind down.
To anthropomorphize for a minute, millennia of evolution likely recognized this phenomena, and also noted that loading up an immune response is an unfortunately long process. A dendritic cell floating in the blood stream must first recognize + grab onto an antigen, then it needs to crawl into the lymphatic system, and then it hopes to bump into the few naive T-cell that recognizes that specific antigen. Then the adaptive immune response can kick off.
How could evolution optimize this process?
Well…if you didn’t have any priors on when new antigens would come through the door, you wouldn’t care when T cells decided to exit/enter the lymphatic system. When they exit, they are moving to new tissue. When they enter, they are actively looking for dendritic cells to bind to. Perfectly fine to do this randomly in the null case of uniform antigen exposure.
But! If you believe that antigen load is highest in the morning (which is something you can track via the clock genes), it would be smart to ensure that the lymphatic system is bloated with lymphocytes in the morning, removing their ability to migrate into the bloodstream. And according to one paper, that does empirically turn out to be the case in mouse models! Here’s a particularly useful graph:
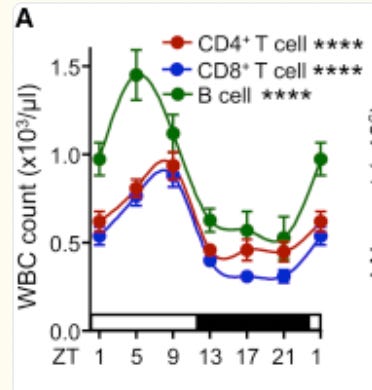
The authors characterize the lymphocytes (T cells and B cells) of mice and find that it is highest during the resting period for mice (ZT 1-9), meaning that they are currently migrating throughout the body. Once the mice get closer to awakening (ZT10), circulating lymphocytes sharply drop, implying that they have moved themselves into the lymphatic system, awaiting for the morning antigens to arrive. Finally, the authors demonstrate that this entire process entirely depends on clock genes. If they are genetically edited out, bloodstream lymphocytes stay constant.
But this is just one immune-circadian tweak that evolution has made. Are there others?
How about prime T-cells such that they are more ‘willing’ to be activated by antigen-presenting dendritic cells at the start of the circadian rhythm? That exists. Perhaps improve the capacity for dendritic cells to migrate into the lymphatic system during points of low antigen exposure/during rest phases of the rhythm? That exists as well. Could we even allow the lymphatic system itself to become more permissible to entry? Technically, this was also a result from the prior paper, so this too exists. Maybe tilt the bodies hormonal signals such that such that immunosuppressive ones are minimized just before expected antigen exposure? Also exists!
Now, what is immunotherapy doing? In the common case of immune checkpoint blockades, it is simply allowing the immune system to more easily attack the cancer, since cancer typically chemically dampens their ability to do so. That’s all it does. It doesn’t provide new antigens, it doesn’t create new T-cell receptors, it doesn’t summon dendritic cells. Which means the effectiveness of that green light depends entirely on what the immune system is already doing at that moment.
Thus, we can propose a decent argument as to why immunotherapies seem to work best during the start of a circadian rhythm. The immune system, by evolutionary coincidence, is simply most prepared to begin their assault during that time.
But you may balk at this and say, “That would only make sense if immune checkpoint blockades had an extremely short half life that fit into this primed immune system period, but they don’t. To take an example, Pembrolizumab (Keytruda) has an extremely long half life of 27 days, is dosed every 3 weeks, and reaches steady-state blood levels at 19 weeks. How could it possibly be affected by initial infusion time?”.
Well, you’ve got me there! I am unsure what the answer could be. And as far as I can tell, so is everyone else, nobody has a clear, consistent answer to the question. But let’s take a stab at it.
Let’s pretend you have very early-stage cancer. The dendritic cells are in their normal cycle of desperately presenting tumor fragments to T cells, the T-cells rightfully getting upset, activating themselves, and going off to hunt the cancer. But cancer simply shuts them down by expressing an immune blocker protein: PD-L1. In response, the T-cell mostly shuts down, wanders back to the lymphatic system, and gets a little bit more ‘exhausted’. It believes that it activated itself for no reason, and thus will require a much higher bar for doing anything else in the future. The more times this occurs, the more exhausted the T-cell becomes, the more unwilling to ever activate again. In the limit, it will simply kill itself. Hence why you need immunotherapy to revitalize these cells!
Now let’s assume you received the immune checkpoint blocker Pembrolizumab at one of the best possible times: 7:30am in the morning, when the most T-cells are in your lymphatic system. Those get activated by the dendritic cells and are now finally able to attack the cancer, the checkpoint blocker preventing them from shutting down. Cancer is being killed! What advantages are you potentially privy to now as a result of the morning dose?
Of course all the ones we talked about earlier:
A greater number of T-cells are in the lymphatic system, so more opportunity to prevent exhaustion.
Dendritic cells are more aggressively collecting cancer antigens, so more opportunity for T cells to be activated.
The lymphatic system is more permissible to dendritic cell entry, allowing more interactions between dendritic cells and T-cells.
And so on.
But, all of this would also eventually happen if you had an evening injection. If we squint, the only downside an evening injection would have is that the highest concentration of the drug (at the moment of injection) does not have access to all of these advantages. But given the clearance rate of Pembrolizumab, only 1.25% of it would have dropped in the 12 hours from the evening injection → following morning. So the morning injection upside entirely stands on this +1.25% drug concentration bump. Either we are missing something, or the sum total of the initial 12-hour-long immune advantages are so high that +1.25% is extremely significant.
Perhaps the second take is genuinely true and answers the story entirely. Lots of immunologically useful things are going on in the morning, each contributing a little bit. As is often the case in biology, there is no singular causal factor for why early-morning immunotherapy seems to help so much, just many small things.
But let’s veer off into speculation. Maybe we are missing something?
Perhaps we’re being overoptimistic on this idea of ‘steady state circulating antibodies’ being useful for T-cell activation. Maybe the first immediate dose of immunotherapy is the primary part that functionally matters for further T-cell activation. This idea was put forwards, albeit only theoretically, in a graphic from this paper.

Which is to say: each wave of activation of T-cells may set as a soft ‘ceiling’ of maximum immune response, even if the drug continues to circulate. So you’d ideally want the first ceiling to be as high as possible, which implies that a morning injection would be best! Is this true? Well, we do know that the clinical impact of the first immunotherapy injection is strongly tied to long term outcomes, and, accordingly, the timing of that first immunotherapy injection seems to matter the most. This same latter paper also says this:
…it appears that challenging the immune system with an antibody at a specific time of day not only changes the quantity but also the quality of the response so that the immune system, once stimulated at the “wrong” time, may not be able to respond anymore to the same level and quality as an immune system challenged at the “right” time—just 12 h apart.
Hence, why we should suspect that there is something fundamentally special about the first wave of activation of T-cells.
Of course, many questions follow from this. What is the temporal “window of imprintability” for T cells? Does that imply that early-activated T-cell clones dominate the final pool of T-cells? And what would mechanistically cause all of this? I don’t have the answer to any of these, and I suspect nobody does.
But again, maybe this is the wrong idea entirely, and there is no singular causal factor for these impressive time-of-day results. Maybe it is, once again, a bunch of small things — increased T-cell activation, but also stronger dendritic cell function and increased lymphatic vessel permissibility and many others — adding up to a strong signal.
For what it’s worth, we do know that this ‘early morning immunotherapy is useful’ phenomenon are also important for infectious disease vaccines, so it feels unlikely that this whole observation is entirely spurious. But vaccines mostly contain short-lived antigens and one-shot adjuvant signals, meaning they rely heavily on getting the initial priming window exactly right. That’s not the case for immunotherapy, so I suspect the benefits of morning injections in that context arise from a different mechanism—one that’s distinct from what makes morning timing valuable for vaccines.
We’ll see what the future holds. The phase 3 trial page that we talked about at the start is still ongoing and is currently the only randomized test of chronoimmunotherapy. But one more is getting kicking off for melanoma and there are calls for more to be run. Incredibly interesting subject, please reach out to me if you have any interesting light to shed here!
Edit on 08/06/2024
At least one person has mentioned that chronotherapy was also thought to matter for blood pressure medication, with rather convincing large retrospective studies, specifically the HYGIA trial. There was some mild mechanistic reason to suggest that circadian variation in sympathetic tone and cortisol levels could influence blood pressure regulation; going up when you sleep, potentially leading to more cardiac events. Thus, bedtime dosing of antihypertensives may prevent the ‘potentially harmful territory’ spike.
But multiple follow-up randomized studies, such as this and this largely disproved the whole concept. Given that, shouldn’t we be on guard for chronotherapy working in immunotherapy?
Well, yes! We should be on guard for everything, especially since our only major piece of evidence is a as-of-yet incomplete trial. But I’m personally erring on the side of the connection between the immune system and the circadian rhythm being much stronger than it is for other physiological functions, just given how large the lymphocyte concentrations in the bloodstream can shift from night to day. I’m also betting a little on the first wave of T-cell activation being particularly important, for reasons that are still not understood. Very open to being completely wrong though!
On a bigger note, someone else mentioned that the clinical trial methodology shifted midway across the 2 years of the study. I asked OpenAI’s Operator to create a table of the biggest changes made:
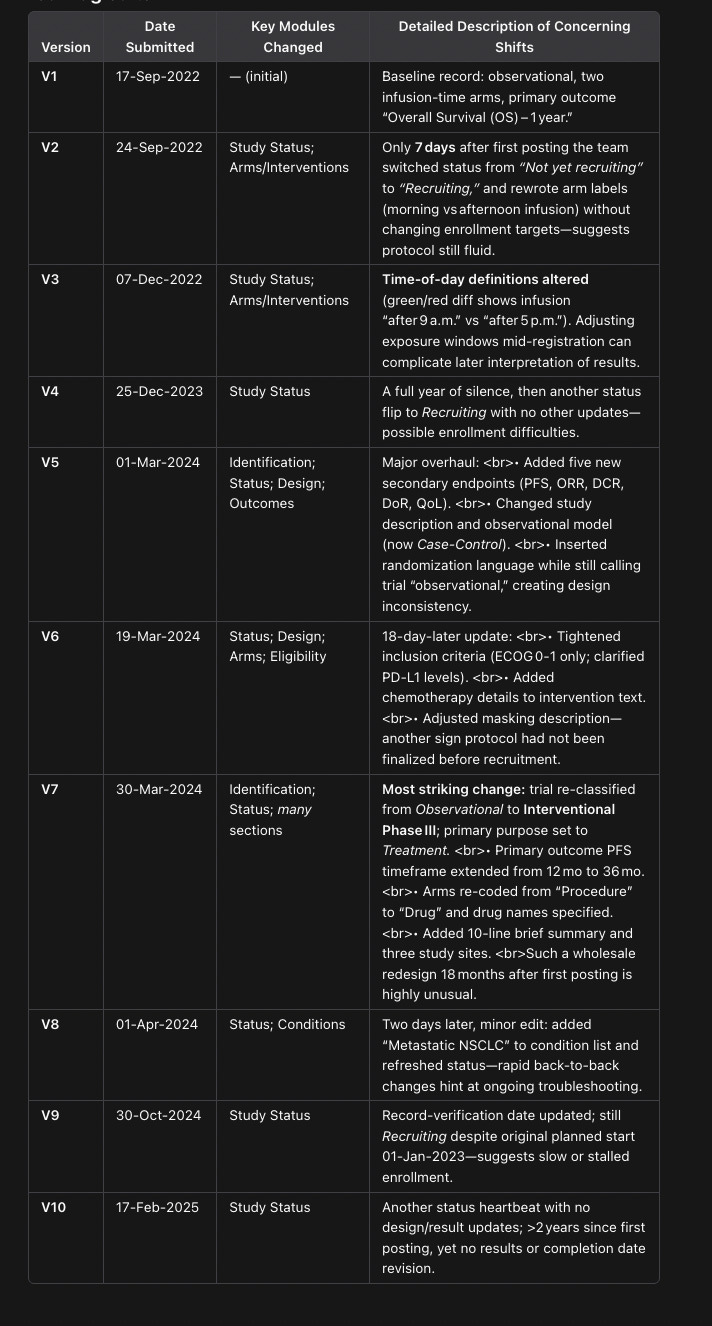
Which matches up with what the original poster says:
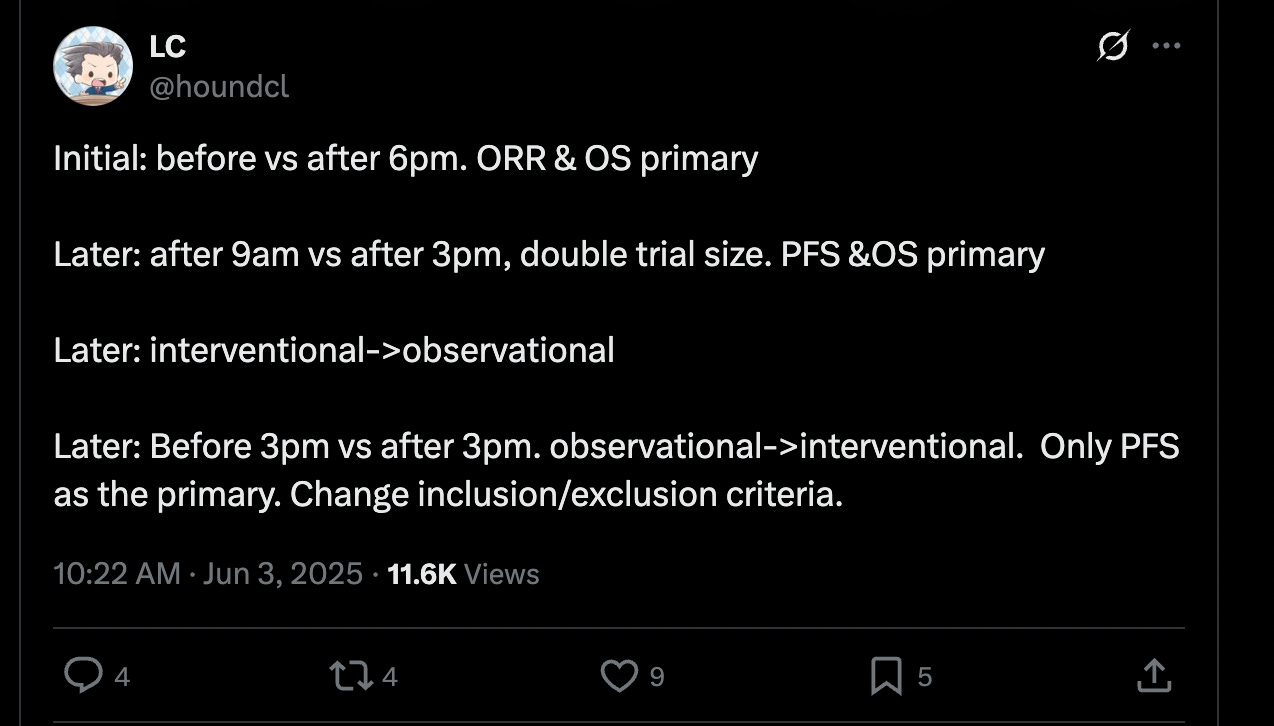
Which is concerning! And perhaps reason to discount the study entirely, mostly for the switch from interventional → observation → interventional. What’s up with that? The fact that it isn’t mentioned in the abstract either is also insane!
But I do consider the timing switches to be only mildly weird. Nobody has really figured out what is an optimal ‘early’ infusion, cut-off times can vary by 4-5 hours. Sure, they shouldn’t have amended it and stuck to one cut-off throughout, but the headline results seem strong enough that I’m not immediately worrying about them gradient-descending their way to a statistically significant result.
Read the original article
Comments
My father was on chemotherapy with fludarabine, a dna base analog. The way it functions is that it is used in DNA replication, but then doesn’t work, and the daughter cells die.
Typically, patients who get this drug experience a lot of adverse effects, including a highly suppressed immune system and risk of serious infections.
I researched whether there was a circadian rhythm in replication of either the cancer cells or the immune cells: lymphocyte and other progenitors, and found papers indicating that the cancer cells replicated continuously, but the progenitor cells replicated primarily during the day.
Based on this, we arranged for him to get the chemotherapy infusion in the evening, which took some doing, and the result was that his immune system was not suppressed in the subsequent rounds of chemo given using that schedule.
His doctor was very impressed, but said that since there was no clinical study, and it was inconvenient to do this, they would not be changing their protocol for other patients.
This was around 1995.
You were obviously on to something and it's frustrating yet completely expected to see all replies with pat dismissals that anything like this gets when there is some real potential innovation in healthcare.
Google 'chronotherapy' with some chemo/cancer/immunotherapy related terms and you'll find a ton of research being done. Given that most of it seems to have evolved in the last 8 years my guess is that the concept was 'vetted' by a nobel prize in 2017 for molecular circadian clock, so people feel safe putting their name on studies in this area.
By refulgentis 2025-06-0922:06 ? The other replies don't dismiss it...
By irrational 2025-06-091:41 Is it the time of day or how long the patient has been awake that matters? It seems like someone could change their sleep cycle to match the doctors schedule if the latter.
As a younger person what are the best habits to get into to maintain optimal long term immune health?
Sleep, exercise, a balanced diet of mostly whole fruits and vegetables, and a moderate amount of whole grains, legumes and fresh meat/fish/eggs if you're not choosing a vegan lifestyle. Avoid ultra processed foods, cured meats, alcohol and other recreational drugs. Make sure you get enough vitamin D, which can be hard with certain diets if you're not supplementing, or getting the right amount of sunlight(latitude and time of year matters).
Try to stay low stress, spend time out in nature, maintain good relationships, etc.
Edit: caveat to spending time out in nature: be vigilant of ticks. A tick-bourne disease can mess up your immune system pretty well
By danbender 2025-06-108:45 Plus, fix your gut.
By FollowingTheDao 2025-06-0914:461 reply Maybe your schema will work for someone who’s on the very top point of the bell curve of human population but human genetic and environmental variability will over rule your advice for the majority of people.
By pinkmuffinere 2025-06-0917:17 The states known for “hippie”/“granola” attitudes, which largely align with the advice given here, tend to live longer than the states that don’t (scroll through the list in [1] to see this). Usually I would insist on a study, but the effect is so striking, and the mechanism by which it would work is so obvious, that I think this simple list is enough. And I’m sure there are studies too, I’m just too lazy to find and link one.
[1] https://en.wikipedia.org/wiki/List_of_U.S._states_and_territ...
By stronglikedan 2025-06-0914:282 reply Don't be a germaphobe. Don't wash your hands a lot. Give your immune system a little work out each day by not babying it.
Try not to take any medicines unless you absolutely need them, and stay away from hand sanitizers. If you do need to clean anything, soap is more than enough and water is usually enough.
I thought it was normal to be over 50 and not take any medicines, but all the doctors and staff were surprised by this when I got my colonoscopy recently.
Above 50? My 30+ year old American friends are all running on pills, daily, many different of them. I was shocked.
So I am rather with you. It should be normal not to take medicines.
By unshavedyak 2025-06-0915:271 reply What sort of pills? Vitamins or ?
By kmarc 2025-06-0915:34 Some yes, and then all sorts of mood boosters, painkillers, etc. Basically all the stuff I later saw during a commercial break at a bar during some sports game. (this should be banned, TBH)
By webstrand 2025-06-0914:38 By hand sanitizers, do you mean something other than the isopropyl-gel based hand sanitizers? If not, I would have guessed that would be little different than using a strong soap.
That said, unfortunately there's some element of luck to it. There's compelling evidence that C-section babies have abnormal immune responses and less diverse body flora. And I imagine childhood circumstance affects things too, city vs country affecting the childhood exposure to pathogens and non-pathogens for training.
By ReptileMan 2025-06-0910:46 Normal weight and enough sleep.
By bregma 2025-06-0915:49 You want to live a long time? Avoid any of the things that make it worthwhile.
By mschuster91 2025-06-0914:42 - Get vaccinated fully and regularly. Any kind of infection is much harder to deal with for the body than a vaccine. Particularly important are the measles and Covid shots, an infection with either of the actual pathogens can wipe out your immune system history and you lose a lot of protection.
- practice safe sex, get tested regularly (even if both you and your partners are exclusive) and get that HPV shot. Yes, even if you're male. Cancer on your bits ain't pretty.
- keep the drug consumption reasonable, especially smoking and alcohol
- the better quality the food, the better your health. Should be a no-brainer and I know about food deserts, lack of time etc
By throwaway290 2025-06-0910:58 Don't compromise it chronically. Protected sex etc.
It’s not shameful, it’s how evidence based medicine works. One case is interesting but not a basis for changing a protocol by itself. Tons of things could have influenced the outcome and you need a proper study to know that.
By AbrahamParangi 2025-06-0823:052 reply The razor to use to determine whether something is actually evidenced based under uncertainty is whether you would follow the same policy if it was your own child.
There are many things that are simply uncertain and “untrue until proven otherwise” isn’t an exclusively optimal policy.
By h2782 2025-06-0911:22 > The razor to use to determine whether something is actually evidenced based under uncertainty is whether you would follow the same policy if it was your own child.
What? This makes no sense. How do you explain anti-vaxxer parents with this perspective? Parents may feel they know best, but feeling and fact have nothing to do with each other.
By raverbashing 2025-06-096:352 reply It's ok, the strongest defenders of EBM are never going to discover anything worthwhile as they get caught in a loop of "no evidence enough to test" and "no evidence for this because nobody tests it"
By ch4s3 2025-06-0915:31 The opposite approach exposes people to a lot of unnecessary and dangerous medical treatment. The evidence based approach has uncovered that stenting doesn't work[1], yet a lot of do something proponents are still installing them at great risk to patients and at great cost to medical systems.
[1] https://lowninstitute.org/stents-dont-work-a-look-back-at-th...
By vrc 2025-06-0912:52 Counterpoints: the detractors of this purported loop would likely neither fund the vast amounts of research they’d demand be done nor believe the results if they conflicted with their anecdata. I have yet to see a good faith argument against evidence based method that provides an effective and realistic alternative. Because that would take evidence.
It is not shameful indeed. One never knows what the father had experienced if he had been given the therapy during the day.
The oncologist could have written a paper (there are many single case papers), or started a trial by himself (requires a lot of organizing) if he was very intrigued. But of course one can’t do that for every above average case.
I have to say, in this particular case there is a very plausible mechanism and the trial would not be that hard. So it is a real shame that nothing was done with this.
By raylad 2025-06-0923:23 Previous rounds of chemo were done on the normal morning infusion schedule and he ended up with a completely depleted immune system and was put in strict quarantine. He also got multiple infections that were life threatening.
This is the reason I started looking into the alternate dosing schedule.
Well the concept is now being studied quite closely. Had someone taken it seriously thirty years ago it's quite possible that the net amount of suffering that millions of patients have endured since then could have been reduced.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9599830/
I'm comfortable calling that shameful. Not on any one in particular, it's a systemic problem that could be reduced with sufficient tenacity and courage to take risks.
There's limited time and a finite supply of doctors and researchers. They can't study everything that's promising all at once, and good ideas fall through the cracks all of the time.
By JamesSwift 2025-06-0916:251 reply I think this clears a bar of things that are useful and simple to study. Theres basically no effort involved. If it ends up beneficial we just update job postings from 'daytime infusion tech' to 'nighttime infusion tech'. Instant improvement in outcomes. I doubt you even need to clear this in any way to get the study greenlit.
By jcims 2025-06-1114:22 Agreed. Scheduling is patient discretion anyway. It's the lowest bar possible as far as I can tell.
By refurb 2025-06-0917:14 > Had someone taken it seriously thirty years ago it's quite possible that the net amount of suffering that millions of patients have endured since then could have been reduced.
You can only say that with hindsight because of the data over the past 30 years.
What if the data showed the opposite? Then the doctor would have given his patients a worse outcome all on a "hunch".
> It’s not shameful, it’s how evidence based medicine works.
Yeah, but I'll bet nothing happened as an outcome of this. No study, no communication to anyone else. That information probably just withered on the vine.
I did a molecular bio undergrad and had classes with a bunch of pre-med students. They had zero interest in the science, just getting A's. They did care about appearance and money, driving cool cars, and dating hot partners. I know my experience is purely anecdotal and not indicative of all doctors, but I came away from my undergrad experience highly unimpressed with our medical feedstock. The only students in upper level electives that cared were the research-track students.
I talk to my doctors regularly about medicinal chemistry and biochem -- they don't know anything. It's embrassing how little they retain or care.
"Evidence-based" is a really problematic term when it is used to protect bureaucracies and medical managerialism, rather than actually interact with scientific processes in an ethical way. Their anecdote is actually a good example of why evidence-based logic is not the end-all.
By uselesswords 2025-06-0912:032 reply [flagged]
By manjalyc 2025-06-1012:35 Prof. Barry Marshall is an example of why Evidence-Based Medicine works against community sentiment.
By uselesswords 2025-06-0917:421 reply [flagged]
By uselesswords 2025-06-1012:04 Since no one wants to explain and you I just got downvoted, Barry James Marshall is ironically an example of EBM and is HIMSELF an active proponent of EBM.
He had a biological hypothesis that the scientific community disagreed with and tested it on himself for a case study to get data. That case study was successful and then became a clinical trial. That trial was replicated and shown to work. He then won a Nobel prize for that work and the risk he took. This is an evidence-based process. EBM doesn’t mean you disregard a N=1, it means you expand N=1 into N=10, then N=100,… before you apply something to the general population. This is loosely how phase-1,2,3,4 trials work in the US.
Dismissing EBM because of Marshall is like dismissing all of math because someone disproved a popular conjecture like the local-to-global conjecture. Sure the community sentiment had it wrong, but the systematic logical approach of Math got it right. In Marshall’s case the community sentiment had it wrong, but the EBM approach eventually got it right. Half this thread doesn’t even know what they are arguing against.
By uselesswords 2025-06-1010:462 reply [flagged]
It's great that you're in medical school and very aware, but that doesn't make it ok to break the site guidelines, which you unfortunately did repeatedly in this thread.
If you wouldn't mind reviewing https://news.ycombinator.com/newsguidelines.html and taking the intended spirit of the site more to heart, we'd be grateful.
By uselesswords 2025-06-1714:051 reply Sorry, I was definitely snarky in my comments and if I could edit my comments to remove the snark and change the tone I would.
However, your "It's great that you're in medical school and very aware" is very patronizing and pointedly dismissive. Its a superficially polite acknowledgment that feels sarcastic rather than genuinely complimentary. I don't really mind, and I acknowledge the point you're trying to make. But if your goal is to curate a curious discussion and avoid snark you should model it too.
By dang 2025-06-1817:13 Sorry! You are right.
It's all too easy to fall into, and we do it too. In such cases it's good when people point it out, and I'm happy to take my own medicine.
The fix is to be more mindful of how easily this happens and edit one's comments to err on the side of unsnark. That's what I will do. If you're willing to do that as well, then HN will be better off in both cases.
(I do think it's great that you're in medical school and willing to share some of what you know on HN, but I shouldn't have singled out the "very aware" bit - that was me being passive-aggressive.)
By dang 2025-06-1319:53 You crossed repeatedly into personal attack in this thread. That's not ok and not allowed here.
If you wouldn't mind reviewing https://news.ycombinator.com/newsguidelines.html and taking the intended spirit of the site more to heart, we'd be grateful.
By uselesswords 2025-06-0911:58 Here’s my anecdote for your anecdote. While there certainly are doctors who care about the flashy lifestyle, I know plenty more who truly care.
Also medicine is an evidence-based practice because fundamentally our knowledge is woefully incomplete. Doctors are basically applied statisticians, the chemistry and biochemistry people are the researchers.
Sure, but someone needs to fund, organize, and conduct the study. If you're not at a research hospital it's not as easy for a one off case to generate a study.
By vlovich123 2025-06-0821:141 reply This is a fairly innocuous change the doctor should be organizing on their own to publish a pilot study. In terms of funding very little would be required since you’re just making a small adjustment to when an existing drug regimen is happening which you already isn’t a controlled factor requiring FDA oversight or anything.
Even simple studies are expensive and difficult. You need IRB approval, data collection and organization, staff to do those things. It seems simple from the outside but making it happen takes time, effort, and money which then means also applying for grants which is a process in and of itself.
By vlovich123 2025-06-093:282 reply If a study like this needs a complicated IRB approval or extra data collection vs what’s already being collected for health records, you’re doing it wrong and the process has become more important than the problem you’re trying to solve.
By owenthejumper 2025-06-0912:542 reply What happens if your study clearly hurts people? What happens if your study clearly helps people? You find out in the first few weeks, what do you do? How do you ensure you collected enough of a sample of a general population to make your study representative? How do you ensure your patients properly consented to the study (past shameful human experiments aside, you likely need many institutions participating, so you can't control everything yourself).
Do I keep going or is the IRB approval process clearer now? There is a reason it exists.
By Panzer04 2025-06-0913:39 We can appreciate that process is important, but at some point you're falling down a slippery slope here, surely?
We're talking about a factor that no one has previously had reason to consider important.
Of course, I don't know hard it truly is to undertake a study. I have to imagine for something like this you could write up a basic study protocol in fairly short order.
By vlovich123 2025-06-0914:251 reply I think once again - when the process becomes the metric it’s insane. What time things are being administered is already random and not regulated or organized. “What if it hurts” isn’t relevant for something like this because the reasoning is that the baseline is that “when” doesn’t matter, you’re still giving the same dosage. “What if it clearly helps?” What if. Then you publish a paper or give a talk at a conference and try to better mobile the medical community. Or see if the administrators are willing to help scale this up further.
> How do you ensure you collected enough of a sample of a general population to make your study representative?
You don’t need to. This would be a pilot study to check whether there’s maybe a there there before you do it larger scale to measure predictive power at population level.
> Do I keep going or is the IRB approval process clearer now? There is a reason it exists.
I think you’re completely failing to engage with the argument that this particular case about time shifting delivery of a drug should not need meaningful IRB engagement other than “I’d like to change the time I deliver the drug for 2 more patients because we had one patient respond positively and this isn’t believed to be a factor” “ok cool yup”.
You’ve jumped from no IRB to full IRB without considering the context of the problem being solved which is why I said when the process becomes the goal vs the problem you’re trying to solve - you’re imaging the worst and most complicated situations possible for a case that would never demand it.
By owenthejumper 2025-06-100:501 reply You are approaching things from software development perspective of "what's the worst that can happen? I rollback". In the topic discussed, you cannot rollback. While you might have a reasonable suspicion that changing the time will improve some outcomes in most, you cannot be sure that it won't greatly reduce positive outcomes in many. The IRB is often in place not to stop positive outcomes, but to reduce negative ones.
By vlovich123 2025-06-1015:50 No I'm not. I'm pointing out the time of administration literally is already under the discretion of the hospital. There's literally no recommendation one way or the other and hospitals administer randomly based on what's convenient for staffing (i.e. not a medical decision). A) there's nothing dangerous about taking something your doing randomly anyway and systematizing it. B) there's no plausible way this is even remotely dangerous.
> The IRB is often in place not to stop positive outcomes, but to reduce negative ones.
Research can literally be IRB exempt if it provides minimal or no risk to patients which is literally what this is. Even if you put this in the "minimal risk" category which would be extreme that's still minimal IRB oversight and approval takes ~1-3 weeks.
You're imagining IRB is something it's not even intended to be and then saying it's a reasonable bottleneck in general because of real problems it prevents and thus justified for this specific experiment (where it wouldn't be relevant).
This is top to bottom a failure to follow up - doctor's are overworked & fail to follow up on potential research results because they act more like mechanics.
By dotancohen 2025-06-098:051 reply
This holds true in almost every professional field for which life is on the line. Medicine, class 3 electronics, aviation.> the process has become more important than the problem you’re trying to solve.We have a word for this, which roughly translates to "rule of paperwork". Bureaucracy.
By darkwater 2025-06-099:31 And I think there is a reason why the bureaucracy exists in these cases. "Move fast and break things" doesn't work very well there.
By renewiltord 2025-06-096:132 reply Indeed, as any ethicist worth his salt would argue: we don’t want anyone saving lives without proper approval.
By vkou 2025-06-099:07 Any ethicist worth your salt would presumably have no problem approving experiments that will also cost lives.
There are an endless number of parameters in medicine that can be fiddled with. If an N=1 sample were enough to convince you, all sorts of garbage would meet that pattern.
What a intellectually lazy response.
No, it would be more accurate to say "any ethicist worth his salt would argue: don't make changes that could be harmful based on a hunch"
By southernplaces7 2025-06-102:12 I think it was a bit tongue in cheek, not so much lazy. Also, considering the kinds of gatekeeping and forced "concerns" I've seen some ethicists push forth just for the sake of showcasing their fixations instead of really looking at costs and benefits, I don't think it's far off the mark on reality to argue that medical ethics is worth considerable scrutiny too, and shouldn't hid behind a mantle of being above criticism.
It's no wonder biology hasn't even entered into the punch-card phase.
When I did my bio undergrad I was keenly aware our bodies are just scaled up molecular machines. I was hoping for a future where we'd grow MHC-neutral clonal bodies for organ harvesting.
Nope. We're in the stone age.
By refurb 2025-06-0917:18 It's almost as if your undergrad biology gave you just enough information to make assumptions that aren't true?
The medical journals are filled with studies that "should have worked" and didn't.
Heck, there are a ton of studies that "should have worked" that were harmful.
So much for "we're just scaled up molecular machines".
Move fast and break things in human medicine means unethical researchers maim and kill people, often marginalized people. Nazis, Japanese experimenting on prisoners, Tuskegee airmen syphilis experiments, Cincinnati radiation experiments and many others stand as testament to what ambitious unethical scientists will do to further their knowledge and career. Thus we have strict guardrails that slow down how we do things.
I am close with a few folks in medical research and the broken nature of the system and sheer amount of red tape has broken their dreams. It is impossible to get anything done.
There is a difference between "reasonable guardrails" and suffocating progress until it's nearly impossible barring Herculean efforts by multibillion dollar entities. It cannot be understated how badly the current bureaucracy has destroyed medical progress.
We are seeing the same problem with nuclear overregulation result in worse outcomes and more deaths for people globally.
There is real suffering and a human cost, measurable in lives, to slowing down progress - just as there is one for reckless progress.
I don’t disagree but the guy below you wants to grow human shells and try head transplants.
By short_sells_poo 2025-06-0910:47 This is why we can't have nice things. I don't (mostly) doubt that poster's good intentions, but it takes only a few people with undirected ideas and flexible morals or empathy to necessitate strict rules around medical research.
By lofaszvanitt 2025-06-0912:13 good! old, dinosaur like systems need to be forgotten already.
Transplant a few heads and suddenly you never get invited to another Christmas party
By tomcam 2025-06-1115:41 I maybe wouldn’t put this on my LinkedIn
We've been able to clone mammals for 30 years and haven't acted on it. We're still toying with molecular systems beyond the limit of detection.
Clone humans. Cut off their brain stem during development. Turn off cephalization signals for good measure. Scale it up to industrial scale.
Research problems solved.
We'd have every study at our fingertips. We'd have organs and tissue and blood for everyone.
We could possibly even do whole head transplants and cure all non-blood, non-brain cancers.
But we're playing in the sand.
By nothrabannosir 2025-06-097:021 reply This comment, more than any other, has sold me on the value of red tape in medical research.
Our genome is a machine, from the nucleotides to the packing, to the enzyme activity, to the metabolic flux.
Our bodies are bigger machines made of lots of little machines.
Our minds or conscious egos or "souls" are the neurotransmitter and activation activity of the connectome and all of its cells and synaptic weights and metabolic activity. They're our lived experiences for as long as our brains can function. Minds experience and produce wonderful things.
If you divorce the body from the mind, there is no "person". Just a very complicated machine. A very valuable machine full of parts.
A human body in a vegetative state is not a person. It's a dormant machine. People may have emotional attachment to that vestige, but it is no longer capable of being a person. It is not a person.
We use brain dead humans for organ transplant all the time. If you understand the premise, then it isn't that far-fetched that we might grow vegetative humans in a lab for medical use and research.
Bodies that never have brains can never become persons. They're no different from plants.
By willguest 2025-06-098:46 My guess is that you're either a dev or an orthopaedic surgeon, well-versed in managing the machinistic aspects of systems, but with little motivation to go beyond them.
There is decent experimental evidence to demonstrate that we are more than gene expression and the machine analogy you insist on is not a good one for understanding biological systems - see work by Michael Levin, as example.
There is a wider paradigmatic shift underway that moves from thinking about parts to processes. This refocus on relations rather than objects is very important and, for biological systems, points to a fundamentally social/collective aspect to their nature.
The machine metaphor also fails when you can no longer explain how the machine works. This is true in many areas of medicine (e.g. anasthesia) and, while we continue to believe (sometimes with enormous zeal) in the concepts that helped us in the past, we cling to them at the cost of building better understanding.
What you say isn't "wrong", but it is too limited to be a useful guide in asking new questions about things like immunotherapy treatments.
You might be surprised at how little of the body still functions without brain function, well, some bits of the brain, including basic homeostasis and immune system function.
We're not at all trying.
If you toss out the old rule book and provide unlimited funding, it can be made to work.
By darkwater 2025-06-099:35 Yeah, sure. There are probably going to be only a few tens of thousands "unknown unknowns" side-effects but hey, who cares? We will figure them out, we are out of the stone age cave now!
By daveguy 2025-06-090:31 That's why doctors publish case studies all the time -- to inspire larger scale and statistically sound studies.
By more_corn 2025-06-0823:21 Or you could consider if there’s reason to believe there’s a causal relationship, if there is you could change your protocol (offer it in the evening as an option), measure the improvement, publish the result and simultaneously improve your patient outcomes and move science forward.
> And shameful (for them.)
1. A single positive outcome with N=1 should generally not be the basis for making a medical recommendation.
2. It takes a mountain of research work to go from that to a study that you can draw meaningful conclusions from.
3. The hospital is not in the business of doing research, it's in the business of treating patients.
Regarding 3: Shouldn’t the medical system be optimizing for patient outcomes rather than the business their in?
Regarding the first two: I think the anecdote being from 1995 suggests there would have been time to put together said mountain of research.
I’m not agreeing that this is shameful for the original doctor, but I do think it’s shameful if avenues for potential research are not taken because it’s inconvenient for the hospitals.
It is at cancer centers. Community oncologists don’t have the resources to do it.
Example: https://www.medicalnewstoday.com/articles/cancer-time-of-day...
By raylad 2025-06-0923:25 This was Sloan-Kettering.
They gave morning infusions because it was convenient. To get my father the evening infusion we had to hire private duty nurses to come to his apartment.
By vkou 2025-06-0823:08 Yes, it should.
But cost is also important to patients. Or it would be in any universe that made sense.
1. The N=1 positive result isn't the sole basis for expanded effort. The basis the is the compelling, research backed, causal mechanism that predicted the scheduling adjustment's success.
2. Does it? Speaking directly out of my butt here (not in healthcare, not an academic), but the OP spoke of pretty acute symptoms specific to a treatment plan. If the treatment program is at all common, then a very straightforward A/B split of non-intervention / intervention.
Heck, even a questionnaire of past patients cross-referenced with historical records of appointment times could go a long way to validate the hypothesis.
3. This degree of specialization is for insects. If literal MDs in the field are too atomized to even surface research proposals, then that feels like an awful waste of edge-research capability.
And if the A/B test says that your intervention made the situation worse? Now the doctor is held liable for that.
By s1artibartfast 2025-06-0919:18 Not how it works. Doctors have wide latitude to treat patient based on their personal medical intuition. You already have doctors dosing patients at all times of day. If an A/B test shows evening is optimal, all the morning administrators will not suddenly become liable retroactively. Hell, they wont even be liable if they keep doing it in the morning because it fits their schedule better.
By vlovich123 2025-06-0821:151 reply I agree n=1 generally isn’t enough, but something like this is easily something you ask for volunteers for as an experiment. There’s 0 risk, you’re taking the same drug. The only reason a given time is selected anyway is for administrative ease not because there’s medical requirements.
By vlovich123 2025-06-093:301 reply Clearly they did it for one patient and it was a good result. Doctors and staff generally care about their patients and given there’s plausible scientific reasoning why this worked, they’d help figure out how to make staffing work for 3-5 more patients for a limited time. Additionally, positive results like this start to travel by word of mouth so if this is successful it means more funding for the hospital and more patients seeking care from them. That’s how it should work but bureaucracy of medical care is typically resistant to things like that.
In any medical system in the world, you'll find that staff scheduling is the singular, most important constraint for patient care.
That they did it for one patient does not mean that they can do it for everyone - especially when it's not clear if it actually helped, due to a small sample size.
By vlovich123 2025-06-0914:19 I didn’t say everyone. I said do it as a pilot for 2-5 more patients so that you don’t write it off as a fluke, then give a talk at a conference. If you’re having good results then you can talk with the administrators how to make this a more serious program if there’s actually good results and desire to scale this up.
Nowhere do you start from 0 and go to 100. You take baby steps scaling up to see if the results hold.
By raylad 2025-06-0923:26 I posted this above, but for clarity:
This was Sloan-Kettering.
They gave morning infusions because it was convenient for them.
To get my father the evening infusion we had to hire private duty nurses to come to his apartment.
Given the scheduling was clearly not based on a medical recommendation in the first place given they were prepared to change it, then even a single datapoint suggesting it might have an impact should be reason to do at least minimal investigation into whether #3 might be better served by altering the schedule.
Since they clearly could alter the schedule, offering a limited number of later slots and comparing results would seem like the prudent response.
> Since they clearly could alter the schedule, offering a limited number of later slots and comparing results would seem like the prudent response.
There's a difference between a doctor entertaining a medically-irrelevant suggestion from a patient (or patient's family), vs. assuming that the subsequent improvement was related to it, and then making that decision for some other patients (or suggesting it to them). The former is being accommodating, the latter is making treatment changes without good reason.
Improvement or no change aren't the only two possible outcomes for a patient. They could also get worse. What's worse, often neither improvement nor decline are obviously related to the treatment, or treatment changes.
Maybe it's the circadian rhythm thing. Maybe it's some delayed effects of something unrelated about the patient, that just coincided with your intervention. Maybe it's just a response to a change - any change. Or maybe it's just completely random. The point is, you don't know. You might feel like you do, or maybe it really looks obvious - but from N=1 you don't actually know, not enough to potentially bet other people's health on it.
Because maybe you do go ahead, and make a schedule change to another few patients - and few days later, suddenly and for no apparent reason, one of them goes into critical condition and dies soon after. Good luck convincing the grieving family, your colleagues, the board - and your own conscience - that the schedule change could not have possibly caused this. You won't, because you don't actually know.
They are already making treatment choices without good reason when they set or change the schedules.
They could already have made it worse with prior scheduling decisions, without having any idea.
Intentionally choosing to ignore a possibly harmful effect of the current lack of scheduling rules seems to me as blatantly unethical or worse as taking reasonable steps within what is already permitted to try to address a possible negative effect.
If concerned about making the schedule change for them: Provide the option. Add appropriate warnings if you like.
But also consider that any grieving families that finds out after the fact that there might be a known benefit to changing the scheduling would be equally hard to convince that you've not acted unethically and done harm.
By TeMPOraL 2025-06-108:29 > They are already making treatment choices without good reason when they set or change the schedules.
In a sense, yes - but there's a difference between following established protocol or understanding, vs. changing it; the difference comes from operating under extreme uncertainty. It's a version of "if it ain't broken, don't fix it" - especially if you're not able to fully commit to identifying the problem, devising a fix, and verifying it's actually doing what you expect for reasons you expected.
> They could already have made it worse with prior scheduling decisions, without having any idea.
Or they could've made it better without having any idea. Point is, they had no idea either way.
> If concerned about making the schedule change for them: Provide the option. Add appropriate warnings if you like.
Even providing an option is already biasing the patient's decisions. Especially in matters of health, people will happily ignore all the warnings you can give (especially if they're mostly philosophical points about ethics or epistemology) and grasp for anything that could help. They're not going to be making a calm and objective choice. Doctors are fully aware of this, and with that awareness, presenting an option is really making a decision for yourself, but dumping any potential fallout on a patient. It's the 21st century, we know what informed choice is, and that wouldn't be it.
> But also consider that any grieving families that finds out after the fact that there might be a known benefit to changing the scheduling would be equally hard to convince that you've not acted unethically and done harm.
For better or worse, that's a big part of what evidence-based medicine is - a shield to protect you in situations like these. It lets you say that "might" wasn't enough - that the benefit wasn't actually "known", but merely anecdotally reported; that the benefit could be real, or could be coincidence, and there could be drawbacks too, unknown or under-reported (so the family didn't stumble on anecdotes of failure like did on anecdotes of success). It lets you say that there is an actual framework for evaluating what's ethical under uncertainty, and it deemed the risk too high. Most importantly, it lets you say all that, and have the entire medical community back you on this. Whether or not your conscience agrees, at the very least the will judge you as acting ethically and in best interest of the patient.
EBM and standard protocols are far from perfect - but they have solid ethical and epistemological grounding, and achieve the goal of minimizing harm to the extent possible under extreme uncertainty the medical field operates in.
By chiefalchemist 2025-06-0823:18 It shameful in the sense we all know there are circadian rhythms. We know the human body is not uniform from waking to shut eye. With this in mind health care therapies should be intentionally administered at various times - as wide as possible; from that perhaps outcomes will vary. You don’t need a study to look for opportunities to optimize a process.
By bravesoul2 2025-06-090:58 What's the p value? 0.5?
By Gravityloss 2025-06-0921:02 I've heard similar things about fasting.
By HexPhantom 2025-06-097:041 reply It's frustrating (but not surprising) that even with a clear positive outcome, the system couldn't adapt without a clinical trial to back it up
By taneliv 2025-06-097:25 Isn't it also quite understandable? Otherwise we risk the new way working well for half the patients and killing the other half, to exaggerate.
By unnamed76ri 2025-06-0818:112 reply I used to be on a chemo drug and had to take folic acid every day to stop it from doing bad things to me.
I had awful ulcers in my mouth from the chemo drug and had been taking the folic acid in the morning. Through forgetfulness I ended up shifting the folic acid to the afternoon and the ulcers went away and never came back.
By tomcam 2025-06-0818:15 Thanks for sharing, and I’m very glad you are here to discuss it.
By HexPhantom 2025-06-097:071 reply How many side effects people just accept because no one thought to tweak the schedule
And to think about how often such things are figured out individually, but go unnoticed, because there's basically 0 chance for the average person to get anyone to do a study on it.
By hypercube33 2025-06-0912:13 My guess on some of this has to do with a few things. Hormone levels vary throughout the day along with immune system activity; My allergies are always worse in the morning than the day. I'm sure time is a huge component in a lot of medical things but I haven't personally seen any studies on this.
Most people also fast at night (sleeping) and are less physically active etc etc.
By unnamed76ri 2025-06-0919:05 I did make sure to bring it up to my doctor in case the idea could help anyone else.
By levocardia 2025-06-0818:471 reply Hazard ratio of 0.45 seems implausibly high, especially when it's just the exact same treatment dichotomized to before/after 3pm. My money is on something other than a real circadian effect: either the result of a 'fishing expedition' in the data, or some other variable that incidentally varies by time of day. Maybe breaking randomization, leaving the drugs out for too long at room temp, etc. If you really believe this is an important and biologically plausible effect it should be a top candidate for a replication attempt.
>some other variable that incidentally varies by time of day.
glucose level? low in the morning, and cancer likes glucose (among other effects of low glucose a cancer site would probably have lower local acidity, and the high local acidity is one of the tools used by cancer to protect and spread itself) .
By levocardia 2025-06-093:142 reply AM/PM glucose differences are probably going to be swamped by mundane stuff like who has a snack before treatment vs. who doesn't. Are you not supposed to eat before immunotherapy? If so, maybe (non)compliance with that requirement is what's underneath.
By maherbeg 2025-06-1017:32 People are more insulin sensitive in the morning too which could correlate with this.
By trhway 2025-06-098:57 i'd think the local acidity (build up of lactic acid resulting from glucose over-consumption by the cancer cells) would take a bit to build back up once glucose ups after the night.
