
Journavx was approved this year. Why did it take so long to develop?
In the nineteenth century, the invention of anesthesia was considered a gift from God. But post-operative pain relief has continued to rely on opioids, derivatives of opium, the addictive substance employed since ancient times. Although no other drug has managed to match the rapid, potent, and broadly effective relief delivered by opioids, their side effects have led to decades of addiction and overdose, leaving researchers keen to find a better solution.
This all changed in January 2025, when the FDA approved Vertex Pharmaceuticals’s Journavx (suzetrigine): the first non-opioid pain reliever suitable for treating post-surgery pain. Clinical trials found no signs of the problematic side effects associated with opioids: no drug abuse, tolerance, or withdrawal. But this was not an easy win: Vertex and other pharma companies spent decades searching for drugs like this to no avail.
Opioids are used primarily to treat nociceptive pain, pain caused by tissue damage from injury or disease. This damage activates nearby nociceptors: sensory neurons that signal physical or chemical harm. These nociceptors send signals up to the central nervous system – the brain and spinal cord – and the brain then creates a localized sensation of pain, drawing your attention to the threat.
Traditional opioids mimic opium, a compound found in the poppy plant that contains morphine. Opioids alleviate pain by acting on one of the three main opioid receptors, mu (μ) opioid receptors, which are distributed throughout the central nervous system, particularly in the brain. When opioids bind to the brain’s mu receptors, this suppresses incoming pain signals from the damaged site’s nociceptors, preventing the brain from creating the sensation of pain even when tissue damage is present.
Our bodies naturally produce their own opioids – such as endorphins, endogenous morphine – to briefly blunt pain during moments of stress or injury. However, these are far weaker and shorter-acting than prescription opioids since they degrade quickly, remain localized, and are released in short, controlled bursts. Prescription opioids, on the other hand, flood the brain with higher doses that linger for hours.
Crucially, opioids don’t just kill pain: they also incite pleasure. When the mu opioid receptors present in the reward center of the brain are activated, this reduces the secretion of a neurotransmitter called GABA, which works to inhibit dopamine-producing neurons. As GABA release declines, dopamine spikes, lighting up the reward center and inducing pleasure.
With the body’s natural opioids, this is fleeting and unproblematic. When properly prescribed, even synthetic opioids are no issue for most patients: under severe post-surgical pain, opioids mostly function to normalize disrupted brain function, dampening any pleasurable effect. But for some, whether due to genetics or inappropriate administration (e.g. a prescription that goes on after the pain’s source has been relieved), the intensity of prescription opioids produces a prolonged dopamine spike, along with a marked sensation of euphoria: a recipe for addiction.
With chronic use, the body’s natural opioid system becomes dysfunctional. Fewer natural opioids are produced and opioid receptors become desensitized. As a result, the patient develops a tolerance, requiring higher and higher doses to even feel normal.
The nineteenth century witnessed the creation of morphine, codeine, and heroin (which was sold over-the-counter), as well as the invention of the hypodermic syringe. By the turn of the century, 15 percent of all prescriptions dispensed in Boston were for opioids, which were used for everything from menstrual cramps to children’s coughs, and as many as 300,000 Americans, or 0.5 percent of the population, were opiate addicts. Anti-narcotics laws proliferated throughout the states, and the medical community expressed concerns about the liberal provision of addictive drugs. These mounting pressures led to the passage of the Harrison Narcotic Act in 1914, which made opium and opiates the first regulated substances in the United States.
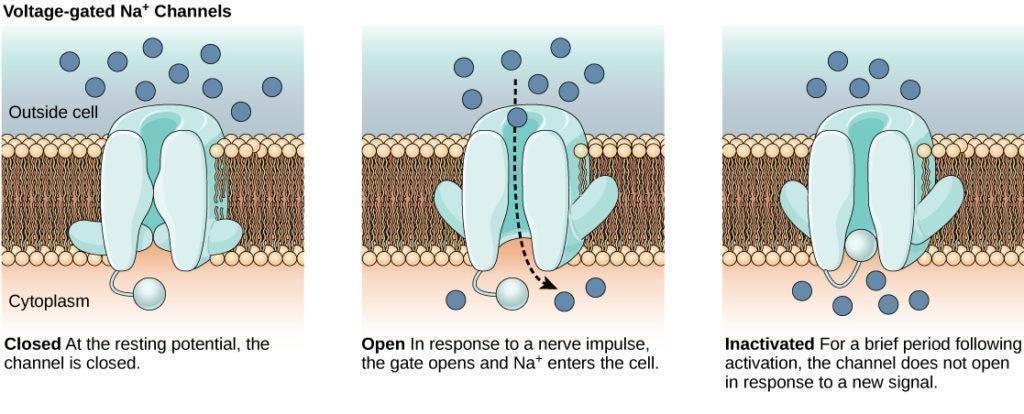
Unlike opioids, which act within the central nervous system, Journavx does not meaningfully interact with the brain. Instead, it targets a specific sodium ion channel found almost exclusively on peripheral nociceptors, the pain-sensing neurons throughout your body. Ion channels, whether sodium, potassium, or calcium, are like tiny doors embedded on the neuron’s membrane: when a door opens, ions rush in or out and the neuron fires, sending an electrical signal to the next cell.
Three sodium channels are found primarily on nociceptors: NaV1.7, NaV1.8, and NaV1.9. Suzetrigine selectively blocks NaV1.8, which stops nociceptors from sending pain signals to the brain. Rather than preventing your brain from receiving pain signals, as opioids do, it prevents your neurons from transmitting them. In essence, Journavx works from the bottom up to alleviate pain, rather than the top down.
Critically, the NaV1.8 channel is largely absent from the central nervous system. This means that suzetrigine does not affect the brain, which means users do not experience the same euphoria that is triggered by opioids. This prevents addiction and abuse, as well as the depressive effects on breathing or heart rate typical with opioids.
At first glance, this may seem like a straightforward solution, especially given the urgent demand for non-opioid alternatives. So why did it take so long?
Unlike diseases with well-defined biological causes, pain is a broad symptom rooted in complex and overlapping pathways. Many of these are deeply intertwined with vital bodily functions like blood pressure, immune response, and respiration. Together, this makes it difficult to isolate a target that can be blocked without collateral damage.
A particularly good example of this predicament involves TRPV1, also known as the capsaicin receptor. It is an ion channel mainly found in nociceptors, and is responsible for the pain you feel when eating spicy foods. In clinical trials, TRPV1 inhibitors effectively alleviated pain, but researchers found that they unexpectedly disrupted thermoregulation, causing patients to experience hyperthermia, or overheating, with one trial participant sustaining a 104 degrees fahrenheit fever for hours.
Another example involves nerve growth factor inhibitors like tanezumab. Although tanezumab alleviated inflammatory pain from conditions like osteoarthritis, Phase III trials revealed an unfortunate side effect: rapidly progressive osteoarthritis. Researchers hypothesized that because patients felt so much better, they overused their arthritic joints, accelerating damage. Although further trials were conducted at lower doses and with restrictions, the FDA ultimately voted against its approval. Tanezumab’s story reflects a difficulty in developing painkillers: while pain can cause excessive suffering, it also serves as a vital warning sign that must be selectively maintained.
Vertex has historically focused on developing drugs targeting ion channels. These channels play a major role in cellular signaling, meaning that compounds that act upon them can produce large, rapid physiological effects. Ion channels are ‘really good drug targets’, Paul Negulescu, head of Vertex's pain program, says, ‘They just require a lot of care and attention to how you measure them’.
The discovery of the NaV sodium channels, made independently in the early 2000s by two different researchers, opened a new frontier in pain research. Both observed that mutations affecting NaV1.7 caused abnormalities in the experience of pain, a major clue that pain might be mediated through that specific sodium channel.
Stephen Waxman, a professor of neurology, neuroscience, and pharmacology at Yale’s medical school, discovered that a community in Alabama had numerous individuals suffering from erythromelalgia or ‘Man on Fire’ syndrome. These individuals experienced mild warmth – such as from wearing a sweater or shoes – as intense burning pain. Waxman’s research tied this phenomenon to mutations in the SCN9A gene, which is involved in the production of NaV1.7 channels. Meanwhile, Geoff Woods, a clinical geneticist at St. James’s University Hospital in Leeds, uncovered a complementary discovery. He observed congenital insensitivity to pain within specific Pakistani communities, also tracing it back to mutations in the SCN9A gene.
This congenital insensitivity provided a particularly compelling genetic validation for a drug target, as the affected individuals were entirely normal except for their inability to feel pain, unlike prior similar cases. Related channels like NaV1.8 and NaV1.9 were also investigated by Woods’s team and found relevant for pain signaling.
But despite the initial enthusiasm surrounding these discoveries, researchers soon encountered significant obstacles: NaV1.7 inhibitors failed to relieve pain during clinical trials. Researchers eventually uncovered that the congenital absence of NaV1.7 did not eliminate pain signals but instead amplified the production of natural painkillers called enkephalins. They concluded that completely blocking the channel, which would be required to replicate this effect pharmaceutically, was impractical.
So researchers turned their attention to the other promising sodium channel: NaV1.8. Again, research began with setbacks: in 2015, it was discovered that individuals with Brugada syndrome, a disorder characterized by abnormal heart rhythms and sudden cardiac death, also had mutations in the gene encoding NaV1.8.
Despite this challenge, researchers still thought NaV1.8 had potential. Woods’ research genetically validated it, showing that mutations in NaV1.8 affect pain signalling. Researchers at the University of Alcalá confirmed that mice genetically engineered to lack Nav1.8 channels showed virtually no spontaneous nerve activity after injury – activity thought to underlie certain chronic pains. Additionally, NaV1.8's almost exclusive presence in the peripheral nervous system (rather than in the brain) suggested that it might uniquely limit undesirable central side effects.
As Vertex researchers searched for NaV1.8 inhibitors, they made use of Negulescu’s E-VIPR technology, which enabled them to conduct more than 50,000 tests per day to identify compounds that blocked NaV1.8 without affecting other ion channels. This was essential because the human body contains nine known voltage-gated sodium channel types, each with a distinctive ‘personality’ – a unique pattern of rapid opening, closing, and voltage sensitivity – making high throughput key to pinpointing an appropriately selective drug.
But even with this tool, Negulescu described the iterative learning process as ‘painful’. Vertex spent a decade screening millions of compounds before finding a promising class of molecules. Another decade was spent on optimization, conducting tens of thousands of screenings to maximize potency and selectivity (a drug is selective if it binds only to the target proteins and nowhere else).
Vertex faced several failures in preclinical and clinical testing. Between 2018 and 2022, they terminated development for three generations of NaV1.8 inhibitors, VX-150, VX-128, and VX-961, due to dosing and tolerability issues. However, unlike previous attempts with NaV1.7, TRPV1, and nerve growth factor inhibitors, the pathway overall did not exhibit fatal flaws, and so research continued.
Eventually, this iterative process produced VX-548, which was discovered to be many times more selective and potent than earlier candidates. In 2022, two Phase II proof-of-concept studies yielded positive results. In 2024, Phase III trials validated VX-548’s efficacy in treating acute pain with minimal adverse effects. During this process, the FDA granted VX-548, now suzetrigine, Fast Track and Breakthrough Therapy designations, processes designed to accelerate the development and review of crucial pharmaceutical innovations.
On July 30, 2024, the FDA accepted Vertex’s New Drug Application, filing it under priority review. Exactly six months later, on January 30, 2025, it was approved, marking suzetrigine – sold under the brand name Journavx – as the first non-opioid analgesic for treating acute pain.
Journavx isn’t a silver bullet. It has not yet been tested or approved for treating chronic pain, from which over 20 percent of Americans suffer. Across its clinical trials, 85 and 98 percent of participants were female. This reflects a broader pattern in painkiller trials, which often rely on surgical models like bunionectomy and abdominoplasty (‘tummy tuck’) – procedures overwhelmingly performed on women. Since 2022, the bipartisan ‘No Pain Act’ has mandated Medicare and other government health plans to cover this class of medication in outpatient surgical settings, private insurance coverage is still in flux: without insurance, a week’s worth of Journavx costs around $230, compared to $10–20 for a low-dose opioid-acetaminophen combination medication.
Journavx failed to outperform that opioid-acetaminophen combination in clinical trials. Todd Bertoch, an anesthesiologist involved in suzetrigine’s Phase III trials, explains that the drug likely won’t serve as an outright opioid replacement, but the first step on the journey to minimizing opioid usage. If paracetamol and ibuprofen are inadequate for pain relief, Journavx can now be prescribed as the next alternative treatment, instead of mild- to moderate-strength opioids.
It will almost certainly improve: Vertex’s scientists are continuing their decades-long project to iterate and screen for even more potent and selective NaV1.8 blockers. They are also investigating complementarities with NaV1.7 inhibitors. A Phase III clinical trial of suzetrigine for diabetic peripheral neuropathy, which involves chronic pain, is currently underway.
Journavx is the product of 27 years, billions of dollars, millions of molecules screened, dozens of monkeys and rats and data from over 2,400 surgical patients, all distilled into a single 50-mg blue tablet.
Vertex chose to keep funding and pushing forward through decades of work that industry professionals describe as ‘tedious’, ‘mind-numbing’, and ‘painstaking’, a slog driven by slow, incremental progress and frequent setbacks. In exchange, humanity now has its first non-opioid painkiller.
Michelle Ma studies economics at the University of Chicago.
Read the original article
Comments
Colloquially acetaminophen/paracetamol and ibuprofen are "painkillers" but this is in a different class, it's amazing to have something which performs like the opioid pain relief but without at least some of the side effects.
It's the first non opioid painkiller applicable for situations like post operative use.
I'd have loved this after my hernia op, the last thing you need with that is opioid induced constipation.
By billforsternz 2025-06-2611:327 reply Off topic complaint: I am guessing an absolutely massive amount of (admittedly minor in each instance) grief has been caused by the most widely deployed simple, inexpensive, useful and familiar drug unnecessarily having two different names acetaminophen / paracetamol. Finally figured this out this year (aged 64) after previously being confused why I couldn't find any damn paracetamol in pharmacies on my occasional visits to the US.
By theoreticalmal 2025-06-2612:597 reply My wife and I got colds while vacationing in Edinburgh and had a heck of a time before realizing to ask for paracetamol rather than acetaminophen. Also, the rules the UK has for limiting paracetamol purchases to small amount per day are so fantastically stupid.
By atombender 2025-06-2619:57 I'm a big fan of paracetamol in terms of how well it works; does wonders for headaches as well as joint aches. My concern is about the relatively recent findings about potential Alzheimer risk [1]:
> During a median follow-up of 12.3 years, 6407 (3.0%) participants developed new-onset all-cause dementia. Participants who regularly used paracetamol had a significantly higher risk of new-onset all-cause dementia (adjusted HR, 1.18; 95%CI: 1.10-1.26), compared with non-users. However, there was no significant association between regular use of ibuprofen and new-onset all-cause dementia (users vs. non-users; adjusted HR, 1.06; 95%CI: 0.97-1.16).
I don't follow the research closely enough to know if this is reliable evidence, but there are other studies showing the same thing.
Paracetamol also well known as mood-altering, apparently inhibiting empathy [2], which may be part of why it has an analgesic effect. That isn't as scary on a personal level, but imagine a society full of millions of people on paracetamol whose ability to feel empathy has been blunted.
Given how common accidental paracetamol overdose is I think it’s perfectly reasonable.
By southernplaces7 2025-06-2621:042 reply Many very simple things can badly hurt or kill someone who doesn't take a few minutes to not be stupid about using them properly. Legislating with absurdities applied to all anything that possibly leads to completely individual harm because a few people can't take normal responsibility for themselves emphatically isn't reasonable.
By padjo 2025-06-2622:36 It’s not theoretical. On one side of the ledger we have people dying horrible deaths, on the other side we have people who can’t have vast quantities of paracetamol on hand for no particular reason. If you do in fact need vast quantities of paracetamol for some reason, it can be prescribed.
By singleshot_ 2025-06-2623:36 > a few
Fifty thousand hospital visits per year
> isn’t reasonable
Fortunately this is not a popular opinion
I’ve never heard of this particular overdose. In the US it’s completely unmonitored and I’ve never heard of an overdose. I’m genuinely surprised.
“A study of cases of acute liver failure between November 2000 and October 2004 by the Centers for Disease Control and Prevention in the US found that paracetamol was the cause of 41% of all cases” from https://en.m.wikipedia.org/wiki/Paracetamol_poisoning
By yencabulator 2025-06-271:23 From that wikipedia page:
> In adults, single doses above 10 grams or 200 mg/kg of bodyweight, whichever is lower, have a reasonable likelihood of causing toxicity.
10g is 20 pills of the highest strength you'll find in a regular store. Excedrin brand "Extra Strength" is half of that, you'd have to be eating 40+ pills in 24 hours, or 20+ pills per day on multiple consecutive days. Most acetaminophen pills have 100-200 mg of the active ingredient.
You're missing the context:
> Intentional overdosing (self-poisoning, with suicidal intent) is frequently implicated in paracetamol toxicity.[25] In a 2006 review, paracetamol was the most frequently ingested compound in intentional overdosing.[26]
So, it's not that acetaminophen will kill that easily. It's just that of the easily available ways to kill yourself, it's distinctly the one that destroys the liver quick.
By OJFord 2025-06-2617:38 It's unfortunately quite easy to do even inadvertently (not following dosage instructions) - doesn't take a lot.
The reason for the rule though was to combat its use in suicide attempts. They also have to be sold in blister packs here for the same reason, not the big bottles of Tylenol/Advil etc. that you get there (and we used to here) - relatively difficult to take several, requires more preparation than just chugging a bottle.
> the rules the UK has for limiting paracetamol purchases to small amount per day are so fantastically stupid
Worse than that: it is effectively per day per shop. In a very short space of time I can buy two packs in Boots, two in Tesco, two in Sainsbury, ooh look another small Tesco I'll get two there as well, two from Savers, two from SuperDrug, …
By delusional 2025-06-2615:411 reply Worse in what ways? I think it's a pretty neat feature of the design. If you just need some, you don't get a lot, and you don't get to buy a lot "just in case". If you truly need a lot, you can go though the hassle of going to multiple stores.
It's essentially just raising a barrier for (under normal circumstances) undesirable behavior.
By oakwhiz 2025-06-2618:48 I think being able to buy a lot of medicine just in case is an amazing feature that makes me less dependent on the supply chain.
By hn_throw2025 2025-06-2615:19 I did something similar when the whole household was coming down with Covid...
And yet the policy appears to have been effective in reducing overdoses.
By dghlsakjg 2025-06-2616:11 Overdoses declined in the US, as well, where there are no limits on quantity, but there has been a campaign to educate and create better labeling practices for medication containing acetaminophen.
I think it's important to recognize that overdoses can be intentional or unintentional, and it isn't clear which ones will be affected by the policy of limiting purchase quantity per transaction.
Based on what?
The US went with the educational route - any product containing acetaminophen has “CONTAIN ACETAMINOPHEN - DO NOT COMBINE WITH OTHER PRODUCTS CONTAINING ACETAMINOPHEN”
Overdoses went down despite the fact I can buy $1,000 tablets for $5 at Costco.
By OJFord 2025-06-2617:39 Based on studies⁰ that examined it.
The fact that another country had success with a different technique too doesn't mean it wasn't successful.
True, but paracetamol overdoses are not a fun death. Granted, you need to take a massive amount, but still.
You don't need to take that much. LD50 is surprisingly close to the normal dose, and possible to do if you don't realise that cold remedies contain it (or that aminocetophen and paracetamol are the same thing!)
By hallway_monitor 2025-06-2613:517 reply I avoid it at all costs because of the possibility of liver damage. Ibuprofen seems to have the same effect without potentially serious side effects.
The drawback of Ibuprofen is that it tends to cause damage to stomach and intestinal linings. That's why you are advised to take with food and/or lots of water. You don't want it absorbing all in one place. Long term use exacerbates the effect, making it more likely to cause ulcers and eventually internal bleeding. My partner ended up in the hospital with a serious internal bleed caused by taking Ibuprofen daily for chronic pain. I'm not saying don't use it, just be aware of the risks.
By lq9AJ8yrfs 2025-06-2616:11 Ibuprofen is possibly worse than that, it seems that it may interfere with sex hormones. [1]
This 2017 study I found in 30s of searching is seemingly underpowered at n=30 or so, but the (preliminary) implication is awful enough that I won't give my boys ibuprofen at all. Out of abundance of caution.
They can have naproxen or acetaminophen instead -- we keep those out of reach and teach our children not to touch them without adults.
Perhaps there is some more recent research?
By colaco 2025-06-2615:34 And also kidney failure in prolonged use, usually in patients with any sort of previous kidney damage.
By ValentinPearce 2025-06-2614:072 reply Ibuprofen is anti inflammatory which paracetamol isn't. IIRC this means ibuprofen can hide infections. I had a doctor friend who avoided its use as generic pain relief for that reason.
By kimixa 2025-06-2623:21 But for muscular/joint pain the anti-inflammatory aspect is a feature, not a bug. And I'd guess that's what most long term user's target is?
By qart 2025-06-2615:35 https://x.com/theliverdr/status/1908363713771425946
Again and again, this hepatologist makes his message clear: "Acetaminophen (Paracetamol) is the safest anti-fever and anti-pain medicine even among patients with liver disease. It is the first choice for fever and pain management even in advanced cirrhosis."
Look for some of his other posts on the topic for studies and citations.
By tecleandor 2025-06-2614:25 People will still happily use paracetamol when drinking or "for hangover" (headache and all that), hitting their liver really hard. :(
By SoftTalker 2025-06-2614:32 I take the OG: Aspirin.
By ChrisMarshallNY 2025-06-2616:01 I know folks that got ulcers; from both ibuprofen, and Aleve.
I take acetaminophen, but only occasionally.
By refurb 2025-06-2617:39 Ibuprofen and other NSAID result in a ton of hospitalizations each year due to gastric bleeding.
By refurb 2025-06-2617:39 The LD50 is 10x the standard dose (5 g vs 0.5 g)
And the people that have serious toxicity at 5 g are likely already sensitive due to alcohol intake, malnutrition, etc.
For a healthy, well fed human who isn’t consuming alcohol the dose that causes serious issues is closer to 20x
By OJFord 2025-06-2616:18 > Also, the rules the UK has for limiting paracetamol purchases to small amount per day are so fantastically stupid.
Its introduction pretty effectively reduced the incidence of suicide attempts by overdose resulting in death or hospitalisation.
https://pubmed.ncbi.nlm.nih.gov/23393081/
(The tl;dr conclusion: it worked, consider going further.)
As annoying as it is (and I agree it is fantastically annoying) much to my surprise admissions for paracetamol overdose to UK hospitals absolutely plummeted after purchasing restrictions were introduced.
Score one for the nanny state.
Not sure what "plummeted" quantifies to in this context, but the US saw meaningful reductions in overdose treatments and calls to the poison control line after changing the labeling rules and a public education campaign. The cited study was even conducted before the full labeling rules change came into effect.
Teach a man why not to over-fish fish vs giving him a smaller amount of fish... or something.
By laughing_man 2025-06-2618:151 reply The US doesn't have a significant problem with deliberate acetaminophen overdose as part of a suicide attempt, which is the problem the UK rules are meant to address.
By dghlsakjg 2025-06-2618:30 Strictly speaking, if you wanted to solve intentional overdoses of acetaminophen, it appears that you could do it by presenting more appealing means of self-harm, like in the US. I'm pretty certain the availability of other lethal products (guns, really) directly correlates with whether OTC drug overdosing is a popular means of harm.
I'm willing to bet that handing out cyanide pills OTC would effectively eliminate intentional acetaminophen poisonings in the UK. Surprised the boffins at the NHS didn't think of it first if they really want to eliminate intentional overdoses! /s
By fifticon 2025-06-2615:55 denmark has same rule, for same purpose and effect
By Marazan 2025-06-2616:51 For those interested having done a brief literature search I've found a review article that paints the picture as much less clear than my categorical statement
> Also, the rules the UK has for limiting paracetamol purchases to small amount per day are so fantastically stupid.
Yes, but:
> Responsible for 56,000 emergency department visits and 2600 hospitalizations, acetaminophen poisoning causes 500 deaths annually in the United States. Notably, around 50% of these poisonings are unintentional, often resulting from patients misinterpreting dosing instructions or unknowingly consuming multiple acetaminophen-containing products.
Source: https://www.ncbi.nlm.nih.gov/books/NBK441917/#:~:text=Acetam...
By tecleandor 2025-06-2614:52 There's an interesting thing too about metamizol. It's very popular here in Spain for some types of pain (for example, teeth related stuff or post-surgery) and it's used widely without much problem. In fact, it was the most sold medication in Spain in 2023 (sold under the Nolotil brand) [0]. But it's forbidden in places like the UK.
Thing is, as we are a popular destination with British tourists or even pensioners that live in the Mediterranean, we've found in the last years that British population is genetically more likely to have a very dangerous side effect, agranulocytosis, that could result in death.
Can't find the exact source (I'm on my phone), but seems like at least half of the metamizol related agranulocytosis cases in Spain have been of British origin, and several deaths have been reported. There's a ongoing legal process where at least 40 deaths are being investigated [1] and doctor have stopped providing metamizol to persons of British origin, and do it carefully for other persons.
So what was perfectly safe around here, was found quite dangerous for certain subset of the British population (no jokes about balconies, please).
Edit for some sources:
From 1998 to 2003, out of the 13 agranulocytosis cases from a hospital in Marbella, 8 were foreigner, and of those 5 were from the UK [2]. According to the ADAF association, out of the 45 deaths attributed to metamizol in Spain since 1996, only 8 of them were Spanish (they don't tell their sources in that article) [3]
--
0: https://fefe.com/wp-content/uploads/2023/05/Obs.-marzo23ok.pdf 1: https://guardian.pressreader.com/article/281857238286709 2: https://www.sciencedirect.com/science/article/abs/pii/S0014256509713104 3: https://www.elespanol.com/ciencia/salud/20231128/denuncian-sanidad-muerte-decenas-britanicos-espana-tomaron-nolotil/812919101_0.htmlI was under the impression that a lot of overdoses of acetaminophen are due to it being included in many different multiple-medicine cold/flu remidies, like cough syrup, NyQuil, decongestants, etc. So people end up exceeding the max dose accidentally when they take acetaminophen along with some of those other things.
Does the UK have rules that prevent mixing acetaminophen with other drugs? Its getting so its sometimes hard to find over the counter cold/flu medicines without acetaminophen
By roryirvine 2025-06-2614:26 The UK rules apply to all medicines containing paracetamol.
Non-pharmacy retailers are only allowed to sell in packs of 16, and they'll usually only allow two packs of any paracetamol-containing medication to be sold at a time (eg. one cold/flu and one cough remedy).
If the name of the product doesn't already contain the word "paracetamol", then all of the packaging must prominently display "contains paracetamol" - so even small retailers that don't have computerised checkouts are expected to follow the same rules.
Deaths from paracetamol overdose fell by 43% (with a similar decrease in the rate of accidental poisonings) in the first 11 years after these changes were implemented: https://www.bmj.com/content/346/bmj.f403
By zdragnar 2025-06-2615:18 My wife has negative reactions to it, which is extremely rare at normal doses (to the point many doctors don't believe her).
Trying to find medicine for her when she's sick is surprisingly time consuming as it is in so many things even vaguely related to treating cold / cough / flu symptoms.
There was no grief in my case. I was recently in Italy with my mother. With a picture of a Tylenol bottle, before I could even utter sto cercando..., the pharmacist quickly gave her a box of something. I think it was called panadol.
By lmpdev 2025-06-2620:35 Panadol is a household staple in Australia as well
By bgeeek 2025-06-2612:17 I have a few prescription medications that are called different things in the US. I thought it was fairly common knowledge with paracetamol, though. Tylenol being one of the common brands names.
By privatelypublic 2025-06-2612:57 Don't forget people like to call it APAP too.
Tylenol also. Virtually all drugs and chemical products go under a bunch of somewhat confusing names. I guess for marketing?
Tylenol is slightly different in this case, as it is merely a brand name widely associated with their most commonly sold medicine. Tylenol does also make other medications, but the majority of it contains acetaminophen/paracetamol.
Acetaminophen and paracetamol are two names for the same generic chemical composition drug, which is why it is especially confusing. You can ask for aspirin or ibuprofen in any English speaking country, and they'll know what it is, but the world is divided on which of the two generic names to use: some acetaminophen, some paracetamol.
FWIW, acetaminophen was coined a year earlier than paracetamol, much like soccer was the accepted term far prior to football, but the Brits and a fair few other countries choose the later versions of the words.
I don't think that is correct re football. Football is an English invention. It then split into Association Football and Rugby football.
From Association Football we get soccer. So Football was first then soccer.
e.g. The Football Association was formed in 1863 and the first international match in 1872 was billed as International Foot-ball Match and then in small writing (Association Rules) before the term soccer was used.
By zdragnar 2025-06-2617:03 Ah you're right, I may have gotten my memory slightly mixed up. Even so, the name soccer (at least as a nickname) was formed in the UK, along with association football, both referencing the same thing, and which became more popular over time diverged across country lines, so the analogy isn't too poorly fitting at least!
By somanyphotons 2025-06-2616:13 I had a really bad first few days visiting the US the first time because of this
Paracetamol is the standard and WHO approved name used everywhere except certain parts of the US. It's ridiculous the FDA chose acetaminophen.
By connicpu 2025-06-2614:32 Paracetamol was coined in 1956, acetaminophen was coined in 1955[1]. The world pharmaceutical stage was a bit less globalized back then, so splits in naming like this just happened. They're both contractions of the full chemical name, so it's hard to argue one is more correct than the other. At this point the names are too entrenched in their respective countries, so changing them would only cause mass confusion and likely overdoses due to people not understanding what they're taking.
What parts of the US use paracetamol? I’ve lived on both coasts and the Midwest and haven’t ever seen anything but acetaminophen.
I've live for all my life in a lot of places in the US and "Paracetamol" was never used. I'd never heard that term until this HN thread.
By closewith 2025-06-2615:47 The overseas territories are split on which variant they use.
By xeeeeeeeeeeenu 2025-06-2610:381 reply >It's the first non opioid painkiller applicable for situations like post operative use.
Perhaps the first approved by FDA, I don't know. In many countries, metamizole is the first-line drug for postoperative pain.
(It should be noted that metamizole may very rarely cause agranulocytosis. It is suspected that the risk varies depending on the genetic makeup of the population, which would explain why it is banned in some countries but available OTC in others.)
By arthur2e5 2025-06-2613:37 From my limited experience of metamizole it feels a bit stronger than paracetamol/acetaminophen. Neat little drug if your genetics can take it.
Tangential: China technically banned metamizole due to the agranulocytosis scare, but somehow small clinics always have fresh stocks of this stuff. And their stocks don't look like my metamizole for horses! It's pressed out of the usual magnesium stearate instead of whatever rock-hard thing they use for animal drugs in China.
By arethuza 2025-06-2610:50 I broke a tooth because of kidney stones...
I had kidney stones last year, by far the most painful thing I have experienced, and got opioid based painkillers which made me constipated. To try and fix that I was eating some stoned prunes and it turns out one of them wasn't stoned and I damaged a tooth (it was weak anyway and needed replacement with an implant).
By nick__m 2025-06-2611:41 I received Ketorolac after a tooth replacement (airbags packs a good punch) and it was more effective than the 5mg baby sized morphine pills they prescribe nowadays.
It's a NSAIDs but it's not to hard on the stomach but it's somewhat hard on the kidneys. However Ketorolac is a dangerous drug if you don't follow the posology (don't take 2 pills at the same time, the therapeutic index is that narrow) or if your a poor metaboliser, it leads to kindey failure, stomach bleeding and other life threatening side effects. I would be surprised if that new pain killer was superior to this.
I am sure it's less dangerous but more effective I really doubt it.
Breaking news: turns out acetaminophen has an active metabolite that acts on... sodium channels.
https://medicalxpress.com/news/2025-06-acetaminophen-discove...
AM404 really is the metabolite that keeps giving. The central nervous system system effects were fun too, acting on cannabinoid receptors and/or TRPV1 channels -- so either stony or spicy.
By PaulHoule 2025-06-2613:46 I can't say it ever made me feel high, but acetaminophen has been long shown to have significant behavioral effects
https://pubmed.ncbi.nlm.nih.gov/27217114/
https://pubmed.ncbi.nlm.nih.gov/32888031/
My primary care doc doesn't want me taking either NSAIDS or acetaminophen so when I get asked at the urgent care what I take for pain I say "Nothing".
I would certainly consider ibuprofen a "painkiller", it works wonders when I get a headache. So the phrase "the first non-opioid pain reliever suitable for treating post-surgery pain" used later in the article should actually have been the title IMHO...
Interesting that for me ibuprofen doesn’t do absolutely anything (and I’m someone that avoided painkillers almost all my life) I take 1g pills and nothing.
Well, not nothing, my stomach clearly doesn’t like it and I feel it.
Human pain and painkillers response seems extremely variable across different subjects.
By unaindz 2025-06-2614:31 My family usually had paracetamol so I went till my early 20s without getting anything for pain or colds as it didn't do anything to me and it felt pointless. I mostly get headaches so discovering Ibuprofen was a life changer. I got a toothache that ibuprofen did nothing against so I tried paracetamol again, still no effects.
By bravesoul2 2025-06-2611:082 reply I also thought about epidural. Is that a non addictive way to give pain relief (extreme yes)
Epidural is surely just the method of administration (into the spinal fluid) where the actual painkiller administered is opioids, though, right?
Meanwhile my understanding of Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) was that they were exactly that by definition - Anti-Inflammatories with pain being reduced by reducing the immediate cause of it, inflammation, not by interfering with the actual mechanisms of pain.
I guess one could consider general anaesthesia (laughing gas, ether, and more modern successors) to be "painkillers" too but they're obviously not quite the same category of thing.
Anyway, I enjoyed the article - it would be interesting to hear the author give their own reasons for not accounting for NSAIDs.
By atombender 2025-06-2620:12 Paracetamol/acetaminophen is not an NSAID, though.
NSAID is effectively a shorthand for COX inhibitor; the term NSAID was coined at a time when the mechanism wasn't fully understood, and all other anti-inflammatories were steroids.
Paracetamol does target COX-2, but does so in a way that doesn't really have any effect on inflammation. Its main mechanism of action is as an AM404 inhibitor.
It is used surgically too (not just in childbirth as you might associate it) but it's a relatively risky procedure vs. a venous injection or pill to swallow.
By Findecanor 2025-06-2611:41 Indeed. After my first bowel surgery, I woke up to a wall of pain — because the epidural did not work. The intense pain caused me to throw up, repeatedly, which put strain on the fresh surgery and the stitches.
After what felt like an eternity, I myself noticed a wetness on my shoulder onto which a broken hose adaptor had leaked. After that was replaced, there were no further issues. Thankfully, the stitches had held, and I didn't get a hernia.
Also, I did have to carry a pee-bag while the epidural was in, because the epidural made me lose control of my bladder. And the epidural itself left a scar.
By johnisgood 2025-06-2613:15 Opioid-induced constipation is easy to counteract, however, with the right form of magnesium, and/or laxatives. There are herbs that you could drink as a tea, too, for constipation.
If you ask me whether I choose pain or constipation, well, I am pretty sure you know the answer.
This constipation goes away once you stop, and everything depends on the dose and the frequency and duration of taking it.
By amalcon 2025-06-2612:20 There are also local anesthetics like the lidocaine family. Some of those are usable for post operative pain in the very short term, but obviously can't be administered orally. That presents a problem for most surgeries, since either they'll want to send the patient home or it's located somewhere that's hard to inject.
By 4gotunameagain 2025-06-2612:154 reply What kind of hernia ?
In the US it seems like they prescribe opioids like candy. I've never heard of opioids post hernia surgery in Europe.
By ggm 2025-06-2621:07 Right Side inguinal fixed with mesh. Yummy post op Opioids, bad constipation advice.
By hn_throw2025 2025-06-2615:271 reply I had open surgery for an inguinal hernia here in the UK. Was sent home with a box of Codeine, 15mg tablets, to go with the Paracetamol.
Plus some sachets of laxative for any constipation.
By 4gotunameagain 2025-06-2618:58 I don't want to be that guy, but UK barely counts in these kind of things, even more so nowadays.
There has been a huge opioid epidemic there as well.
By johnisgood 2025-06-2613:12 In Europe they almost never give you opioids. :|
By stavros 2025-06-2613:14 I got morphine for an appendectomy in the UK.
By aaron695 2025-06-2610:49 [dead]
It will have different side effects.
Plus don't forget: even the "pain relief" provided by sticking a knife through your skin to the bone is addictive. So the side effect of addiction isn't going to go away.
By bheadmaster 2025-06-2610:392 reply > even the "pain relief" provided by sticking a knife through your skin to the bone is addictive
> the side effect of addiction isn't going to go away
While I agree with your conclusion itself, I disagree that the premise implies the conclusion. The main difference between suzetrigine and opioids, as explained in the article:
The "pain relief" provided by sticking a knife though your skin to the bone is caused by endorphine, which functions similarly to opioids, and that's why it's addictive.Crucially, opioids don’t just kill pain: they also incite pleasure. When the mu opioid receptors present in the reward center of the brain are activated, this reduces the secretion of a neurotransmitter called GABA, which works to inhibit dopamine-producing neurons. As GABA release declines, dopamine spikes, lighting up the reward center and inducing pleasure.Since suzetrigine doesn't affect mu receptors in the brain, this mechanism doesn't apply.
But I'm almost sure it will have some other unintended side effects. Morphine had them, heroin had them, methadon had them... And each time the inventors were sure they didn't.
What is this thread? Sticking a knife through your skin to the bone kills pain and is addictive?
Some people pratice self-mutilation to relief their depression. 20 something years ago I frequented a girl who was full of scars under her clothes, she was pretty good at finding plausible excuses for the scars (plausible to a 20yr old ignorant about that practice), one day she confessed that she did this to herself and that she was unable to stop... It's not a memory I tought I would revisit but your question made me think of her and her dangerous mania.
By CamperBob2 2025-06-2621:131 reply 20 something years ago I frequented a girl
LOL, this thread just keeps on delivering.
By CamperBob2 2025-06-271:59 Clumsy? That's a great phrase.
By bheadmaster 2025-06-2611:55 It's a hyperbole.
Injuries generally cause brain to release endorphins, which in turn releases dopamine, causing addiction. For example, cutting is a common type of self-mutilation depressed people do. High-intensity exercise arguably also does the same thing - as your body is "microinjured" by strain, your brain releases endorphins to help with the pain, causing effects like "the runner's high".
By capitol_ 2025-06-2611:27 Maybe they should have said something along the line "replaces the pain with a new one and gives you adrenalin that surpresses it and is addictive"
By TeMPOraL 2025-06-2612:14 "There are more things in Heaven and Earth, Horatio, than are dreamt of in your philosophy."
And the Internet is the place where you get exposed to them at random.
By giardini 2025-06-2617:31 Is this a useful first aid technique?
Like for Aron Ralston, who was trapped under a rock and had to cut off his own leg to escape: would it have reduced his pain if he had stabbed himself in the shoulder to the bone?
Would this best be done with, say possibly, acupuncture needles or an ice pick, so as to minimize the damage and to maximize the relief?
Gunsmoke TV episode:
Doc: Well, Billy, we'll have to amputate your lower left leg - it's shot plumb thru with gangrene.
Billy: Will it hurt, Doc?
Doc: Hell yeah, it'll hurt! But thanks to Hacker News we have a new pain treatment: every time you yell. Chester here will stab your right leg to the bone with this h'yar ice pick. And Mary will hold a leather strap in your mouth so your teeth don't crack off! Don't forget to breathe.
Billy: I'm obliged and grateful to be part of your research program, Doc, but can't you instead just wait 10 minutes while I drink this here quart of whiskey and pass out? Then you can do as you wish.
Doc: Hell, no, time's a'wasting! Hold him down, fellas! Doctorin' progresses only a step at a time!
By circlefavshape 2025-06-2611:14 +1! wtf!
By CjHuber 2025-06-2611:37 It very much oversimplifies the interaction between GABA and dopamine as effects of dopamine and the interaction with GABA varies much depending on the brain region and the specific receptor. Also honestly the conclusion is very much pseudosciencey, if it was so simple nobody would find benzos pleasurable except on withdrawal
I think a better title here than:
> The first non-opoid [sic] painkiller
might be:
> The first non-opioid nociceptive pain-killer
Nociceptive pain being that by actual damage to tissue, as opposed to neuropathic pain like a headache or inflammation that you might take a (non-opioid!) NSAID for.
I'm a neuroscientist by training, and that doesn't match my understanding (although the definitions might have changed).
Inflammation would be an instance of nociceptive pain, and an NSAID would alleviate it by reducing the inflammation; and most tissue damage will result in inflammation.
Neuropathic pain, on the other hand, would be due to damage of the nerves themselves, and NSAIDs are completely useless here (ask anyone with sciatica or other nerve entrapment)
By OJFord 2025-06-2611:53 I'm happy to take that correction - I have no training in any relevant field - I was just trying to follow the description in TFA, which links indirectly to my link above in the second paragraph or so as 'nociceptive pain'; from which I inferred that's all it's talking about and existing non-opioids must therefore not target that.
Perhaps non-inflammatory (or generically) nociceptive pain killing is the point. (Which is getting a bit specific for such a broad title isn't it. Does 'painkiller' ordinarily have such a narrow meaning in your experience?)
By OJFord 2025-06-2611:08 Well my comment will still be here, and at least having the qualifier in the title is a pointer to look it up if needed, or to hint 'oh right ok it doesn't mean of all things, I guess paracetamol does not kill nociceptive pain, whatever that is'.
I guess that would make sense in a scientific paper or journal, but most people would have no idea what that means and just make for a confusing title that would turn people off from reading it. Almost everyone has heard of opiates in the evening news or social media.
By OJFord 2025-06-2613:52 And almost all those people have 'painkillers' such as paracetamol and ibuprofen in their cupboard, which they know not to be opiates.
The point isn't to accurately describe it as 'nociceptive' (which I've never heard of before either) and have that be understood, it's to qualify it such that it isn't confusing or sounding like an historical tale of how whatever the first NSAID/analgesic was came to be.
By badmintonbaseba 2025-06-2613:24 Also everyone heard of pain killers that are non-opioid, so you can't really get around explaining why this one is novel.
By mousethatroared 2025-06-2615:143 reply I think the medical community needs to take more seriously that different people have different pain tolerances.
My wife, daughter and I are very pain tolerant. Out of curiosity, I've turned down freezing for fillings and I even turned down some of pain meds before abdominal surgery. I've never taken the post op opioids, including when I had my impacted wisdom teeth removed.
My other kid, on the other hand, is a whimp. She gets anxious simply if I replace her earrings.
My use case for anesthesia is very different from my kid. I struggle to appreciate why anesthesia is even necessary beyond the need to restrain the patient.
My kid could go into a full blown panic attack from pain.
Yet I don't see anesthesiologists ever asking "how good are you with pain?"
You were born with innate high pain tolerance, but your daughter is a whimp because she didn’t win genetic lottery like you?
I think they're using it hyperbolically. As a parent (who also maybe has a high pain tolerance but I am a guy and we are famous for both thinking that and for not being pain tolerant) my daughter is currently like this including the earrings thing. It's more of a frustration but I know she will grow out of it as she's already gotten a lot better. I would imagine OP is in the same boat and is just letting off a little rhetorical steam.
By mousethatroared 2025-06-2623:431 reply "I think they're using it hyperbolically."
You'd think my comment's thesis that folks with lower tolerances should be respected and treated differently would have given the rhetorical device away.
By janderland 2025-06-271:25 There’s always someone online who will assume the worst interpretation. It’s unfortunate.
wow I'm envious. I remember how much pimples hurt and I was astounded nobody warned me. This now makes me curious what the low pain tolerance to anxiety correlation is.
By mousethatroared 2025-06-2623:29 That the medical community acts as if you and I should be treated the same is insane to me.
By StochasticLi 2025-06-2615:592 reply read some books on parenting
By mrguyorama 2025-06-2620:342 reply My checkbook. It told me not to be a parent.
By tclancy 2025-06-2623:07 And I taught my bevy of child pickpockets to look for old people with checkbooks.
By mousethatroared 2025-06-2623:39 Thank you for forfeiting the evolution game.
By mousethatroared 2025-06-2623:38 Lol, why?
